


{kind=link}
{kind=link}
{kind=link}
OCT血流成像技术的现在与未来
[俞素勤 , 李欣馨, 许迅]
, 李欣馨, 许迅]
, 李欣馨, 许迅]
|
|


光相干断层成像血流成像(OCT angiography,OCTA)是近年来发展起来的一项新的眼科影像检查技术,它通过特殊的运算法则对连续扫描的OCT进行计算,获取血流信号,可快速、无创地重建视网膜、脉络膜血管的三维结构。虽然这种血流成像技术目前尚无法检测眼底血管的充盈时间,也无法评价血-视网膜屏障的功能,但是它已经显示出与传统血管造影基本一致的眼底血管结构,甚至可以更好地揭示视网膜深层毛细血管的形态,发现早期脉络膜新生血管,从而提供更多的病理信息,因此该技术正广泛应用于糖尿病性视网膜病变、黄斑旁毛细血管扩张症、年龄相关性黄斑变性、中心性浆液性脉络膜视网膜病变、视网膜静脉阻塞等多种眼底血管性疾病的检查。尽管这项新技术目前还存在各种局限性,如移动性伪影、浅层血管在视网膜色素上皮层的投影等问题,但是未来随着设备和软件的不断更新,现有技术必将进一步完善,影像会更加清晰而完美,而我们对疾病的认识也会更加深入和彻底。
Optical coherence tomography angiography (OCTA) is a new imaging technology that allows the non-invasive and rapid reconstruction of the three-dimensional structure of the retinal and choroidal vascularization. Importantly, blood flow signals within the vessels can be derived from consecutive scans of the selected areas. OCTA can show vascular structure consistent with conventional angiography, although it cannot yet calculate the filling time and evaluate the function of the blood-retinal barrier. OCTA can reveal deep capillary networks better than ever and detect choroidal neovascularization much earlier, providing additional information of the underlying pathology. Thus, it is now being widely used in diabetic retinopathy, macular telangiectasia, age-related macular degeneration, central serous chorioretinopathy, retinal vein occlusion, and other fundus vascular diseases. Currently, this new technology still has some limitations such as movement artifacts and projection of superficial retinal vessels at the level of the retinal pigment epithelium. However with upgrades in the equipment and software, the current techniques will be improved, providing images more clearly. As a result, we will develop a more thorough understanding of the diseases.
在过去的20年里, 光相干断层成像(OCT)技术发展极其迅速, 从时域OCT(Time domain OCT, TD-OCT)到频域OCT(Frequency domain OCT, FD-OCT); 后者再从谱域OCT(Spectral domain OCT, SD-OCT)到扫频OCT(Swept source OCT, SS-OCT)。就观察角度而言, 既有横断面扫描(B-scan)又有额状面扫描(C-scan)即En face OCT; 就观察内容而言, 不仅有结构OCT(Structural OCT), 更有功能OCT(Functional OCT), 其中OCT血流成像(OCT angiography, OCTA)是近几年发展起来的革命性新技术, 它可以快速无创地重建视网膜脉络膜血管的三维结构, 而无需注射造影剂, 因此迅速地被应用于临床各种眼底血管性疾病的检查[1, 2, 3, 4, 5]。由于OCTA可以比传统造影更好地揭示视网膜深层毛细血管的形态, 发现早期脉络膜新生血管(CNV), 提供更丰富的病理信息, 所以它正改变着我们对很多疾病的理解和认识。未来它是否可以替代传统的血管造影技术, 满足临床需求, 成为眼底病检查的主要手段, 是值得临床眼科医师关注的问题。现简要阐述OCTA的技术原理, 比较当前市场上不同品牌OCTA的设备特点, 重点探讨OCTA的临床应用、目前的局限性以及未来的发展方向。
OCTA的技术原理主要基于一个概念, 就是在静止的眼球里, 眼底唯一运动的结构是血管里流动的血细胞。对同一横断面进行重复扫描(B-scan), 通过特殊的计算方法, 如信号振幅的去相关等, 产生静止性与活动性结构的对比, 从而获得血流信号, 据此进行血管结构的三维重建, 并通常以额状面(C-scan或称En face)的形式逐层呈现[6, 7, 8]。因此OCTA的设备首先就是一台频域OCT, 它可以进行常规组织结构的断层扫描, 但是在传统结构性OCT的基础上添加了功能性的血流信息。
目前市场上各种品牌的OCTA设备主要包括美国光视OptovueAngio VueTM OCTA系统, 德国蔡司ZEISS Angio PlexTM, 日本拓普康Topcon Triton SS OCT AngioTM, 德国海德堡Heidelberg Spectralis® OCTA, 日本尼德克Nidek Angio Scan, 以及日本佳能Canon Angioe Xpert等, 它们各自的扫描模式、算法、眼球跟踪技术、运动修正技术以及视网膜分层定义等都不尽相同[8, 9, 10, 11, 12]。根据各公司公开发布的使用手册、官网上的产品介绍以及使用上述设备研究发表的数据, 我们比较了各种设备的特点和主要技术参数(见表1)。它们有的使用谱域技术, 有的则使用扫频技术。虽然扫频OCT的光源波长比谱域OCT的长, 穿透力更强, 更显优势, 但是由于其技术还处于发展更新阶段, 所以更多用于实验样机, 而临床商业用机多采用谱域技术。OCTA的算法更是多种多样, 包括分频幅去相关血流成像(Split-spectrum amplitude decorrelation angiography, SSADA), 光微血流成像(Optical microangiography, OMAG), OCT血流成像比率分析(OCT angiography ratio analysis, OCTARA), 散斑差异(Speckle variance), 相位差异(Phasevariance), 复合差值影像(Complex difference)和相关制图法(Correlation mapping)等等。其中SSADA是对连续扫描的OCT序列进行相互比较, 但是它将单个B扫描分割成多个频幅, 这样可以减少B扫描的次数, 缩短图像获取的时间, 却又可以提高图像的质量[6]; OMAG的影像对比是基于血管内移动红细胞反向散射产生的光散射信号, 它同时利用OCT信号的振幅和相位变化来显示组织内的血流[13]; OCTARA则不采用基于差异比较的方法, 而是用强度比率分析的算法, 它保留了全频幅从而不损失轴向分辨率[10]。所以各种算法各有其优势。
| 表1 不同OCTA设备的特点及主要技术参数 Table 1 Technical parameters and characteristics of different OCTA devices |
虽然OCTA的检查可以显示出眼底血管的影像, 但是与传统血管造影相比, 存在诸多不同(见表2)。其中OCTA是三维影像, 可以利用En face技术将视网膜分成数层加以展示, 尽管不同设备默认的视网膜分层的参数存在细微的差异(见表1), 但是由内向外大致都可分为:①视网膜浅层毛细血管丛; ②视网膜深层毛细血管丛; ③无血管区; ④脉络膜毛细血管。因此对OCTA影像的阅片也需逐层进行(见图1), 从而分别评估不同层面的血管异常。
| 表2 OCTA与传统眼底血管造影的区别 Table 2 Comparison between optical coherence tomography angiography and conventional angiography |
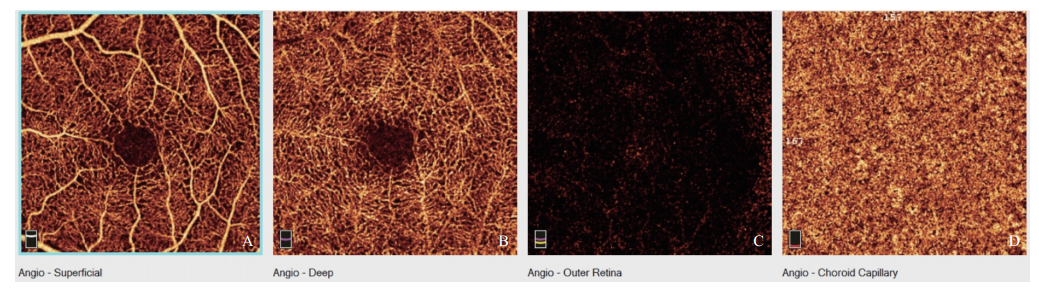 | 图1. AngioVue默认视网膜分层A:视网膜浅层毛细血管丛; B:视网膜深层毛细血管丛; C:无血管区; D:脉络膜毛细血管Figure 1. Default images of the retinal layers by the AngioVue OCTA instrument.A: Superficial capillary plexus; B: Deep capillary plexus; C: Avascular area; D: Choroid capillaries. OCTA, optical coherence tomography angiography. |
OCTA技术一经诞生便被广泛地应用于各种眼底血管性疾病的诊断与观察, 尤其是各种黄斑疾病, 它让我们在不注射造影剂的情况下, 可以清晰地看到眼底血管的形态与分布。
糖尿病性视网膜病变是最常见的眼底血管性疾病之一, 其中糖尿病性黄斑水肿是导致中心视力下降的主要原因。黄斑区血管闭塞导致黄斑区缺血缺氧, 血管内皮生长因子(Vascular endothelial growth factor, VEGF)上调, 最终演变为黄斑水肿, 黄斑功能受损。OCT是目前判断黄斑水肿的重要工具, 可以快速判断黄斑区是否存在视网膜层间积液或视网膜下积液, 是指导眼内注射抗VEGF药物的重要依据, 但是OCT无法显示血管的形态, 所以不能判断黄斑区灌注的情况。而OCTA可以显示视网膜的毛细血管, 并且可以进一步区分浅层和深层的毛细血管丛, 它不仅可以判断黄斑区是否存在血管的闭塞和缺血, 而且可以深入判断是深层还是浅层毛细血管丛的闭塞。目前的研究显示浅层闭塞的范围与深层闭塞的范围并不一致[14]。此外OCTA可以发现比传统血管造影更多的微动脉瘤, 它们有的位于浅层, 有的位于深层, 且深层微动脉瘤的数量往往更多[14, 15]。视网膜新生血管是增殖期糖尿病性视网膜病变的重要特征, 但是传统造影往往因为染料的迅速渗漏而不能很好地显示其具体形态, OCTA不存在染料渗漏的问题, 所以可以很好地显示视网膜异常血管的形态, 但它也因此无法判断血管病理生理的异常, 如管壁的通透性[16, 17]。此外当前OCTA的检查范围有限, 基本以黄斑区域为主, 无法了解周边视网膜的血管灌注情况。
2.2.1 年龄相关性黄斑变性 年龄相关性黄斑变性(AMD)是发达国家50岁以上老年人主要的致盲原因之一, 分为干性/非渗出性/非新生血管性和湿性/渗出性/新生血管性两大类, 前者的主要表现是黄斑区视网膜色素上皮(RPE)的变化和玻璃膜疣的形成, 后者的主要表现是异常CNV生长及由其引起的出血、水肿、渗出和视网膜下积液等。对于干性AMD, OCTA检查发现位于玻璃膜疣下的CNV密度降低, 脉络膜厚度变薄, 在地图样萎缩的区域, CNV血流变慢或消失, 范围甚至超过RPE萎缩的区域, 提示CNV血流的变化可能先于RPE的消失[18, 19, 20]。此外干性还有可能会转变为湿性, 导致患者视力明显下降, 因此密切随访、及时发现异常血管至关重要。传统的血管造影技术往往不能清晰地显示CNV的形态, 尤其是早期和隐匿性病灶, 而OCTA却可以发现早期及隐匿性CNV(见图2), 因此可以帮助我们及时治疗, 阻止病情发展, 保存患者中心视力。不仅如此, OCTA显示的CNV是三维立体的影像, 不同视网膜层面具有不同的形态(见图3), 所以OCTA对湿性AMD的诊断独具优势, 它不仅可以帮助我们对AMD患者的各种色素上皮脱离(Pigment epithelium detachment, PED)进行鉴别诊断, 区分玻璃膜疣样PED、浆液性PED、血管性PED以及混合性PED, 还可以帮助我们判断新生血管的类型, 如1型CNV(RPE下, 包括息肉样脉络膜血管病变PCV)、2型CNV(神经感觉层下)及3型新生血管(即视网膜血管瘤样增生)[21, 22, 23, 24, 25, 26]。由于OCTA可以在任何时候反复检查, 所以在随访过程中更是体现出其明显的优势, 可以实时观察抗VEGF治疗新生血管后的变化和转归[27, 28, 29]。最新研究还发现, 一些晚期相对稳定的湿性AMD患者, 虽然不再有出血渗出, 也没有视网膜层间积液和视网膜下液, 但是OCTA却显示病灶内依然存在血流信号, 提示新生血管已经成熟化, 属于静止型CNV[30]。总之, OCTA的出现让我们对AMD这一疾病的病理有了全新的认识。
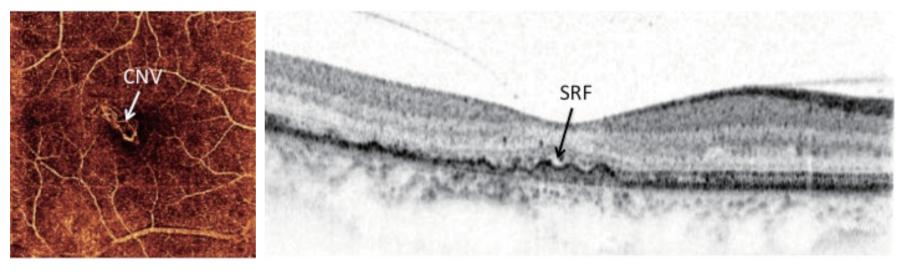 | 图2. 发现早期及隐匿性CNV1名随访多年的干性AMD患者在OCT检查时发现玻璃膜疣的上方出现少量视网膜下积液(SRF, 黑色箭头), OCTA显示已有CNV 生长(白色箭头), 表明干性AMD向湿性AMD转变Figure 2. Early detection of occult CNV.A patient with dry AMD was followed for many years. In a recent OCT examination, a small amount of subretinal fluid (SRF, black arrow) was present over the preexisting drusen. OCTA revealed CNV growth (white arrow), which means that the dry AMD developed to a wet AMD. CNV, choroidal neovascularization; AMD, age-related macular degeneration; OCT, optical coherence tomography; OCTA, optical coherence tomography angiography. |
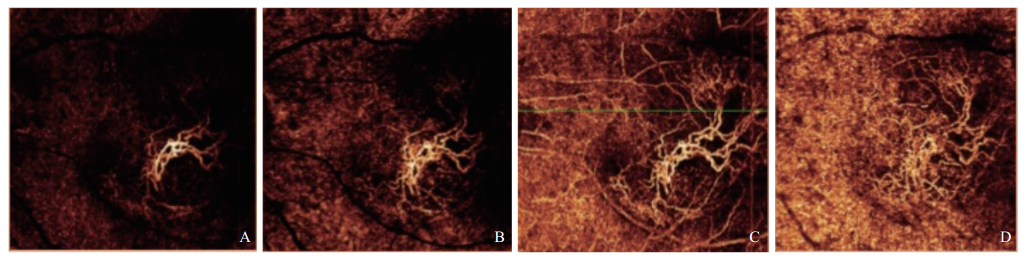 | 图3. 湿性AMD患者CNV的形态从A至D, OCTA显示不同视网膜层面的CNV形态并不相同Figure 3. Morphology of a CNV in a patient with wet AMD. From A to D: OCTA showed that the shape of the CNV varied at the different layers of the retina. CNV, choroidal neovascularization; AMD, age-related macular degeneration; OCTA, optical coherence tomography angiography. |
2.2.2 黄斑旁毛细血管扩张症Ⅱ 型 最初由Gass和Oyakawa描述的黄斑旁毛细血管扩张症Ⅱ 型(MacTel Ⅱ )是一种比较少见的视网膜血管病变, 临床表现为中心凹周围的视网膜透明度丧失、结晶沉积、增生的PRE迁移、黄斑色素缺失、以及黄斑旁视网膜血管逐渐异常等[31]。传统造影检查可以发现病变区域强荧光伴血管扩张, 其他血管异常包括直角静脉、外层视网膜或视网膜下的血管增生等。OCT则显示黄斑变薄, 并在某些患眼中可以观察到内层和(或)外层视网膜空穴, 甚至全层黄斑裂孔[32, 33, 34]。仅有的3例MacTel Ⅱ 患者的眼球病理也缺乏关于此病的一致性描述, 尽管有2例提到Mü ller细胞的丢失[35, 36]。OCTA作为一种非创伤性非介入性检查, 却为我们提供了活体病理生理学信息。检查发现一些患眼的浅层毛细血管密度下降, 但是更为明显的改变则位于深层视网膜血管丛, 轻微的病例可见深层血管膨出和毛细血管扩张, 而严重的病例则可见血管层变薄消失, 残留血管被拉伸、间隙被拉宽, 新生血管代偿性长入视网膜的外层及视网膜下空间[37, 38]。这种视网膜深层血管丛的改变并不能被传统的平面血管造影检查所显现, 而三维立体的OCTA影像则史无前例地将不同层次的血管结构详尽地展示在我们的面前, 并且由此可以推断MacTel Ⅱ 中血管的渗漏与入侵很可能是由于Mü ller细胞丢失失控, 残留血管暴露于视细胞内节含氧更低的环境中而引起的代偿性改变[38, 39]。
2.2.3 中心性浆液性脉络膜视网膜病变 中心性浆液性脉络膜视网膜病变(CSC)是一种常见的眼底病, 临床上以黄斑区色素上皮损害、浆液性视网膜或色素上皮脱离为特征, 目前认为脉络膜血管扩张、通透性增强是造成局部色素上皮损害的原因, 并且与内源性或外源性的皮质类固醇水平升高有关。但是OCTA检查却让我们看到了该病的另一面, 比如OCTA的检查让我们发现了传统检查技术未发现的CNV, 检出率超出我们的想象[40, 41], 尤其是慢性及老年CSC患者, 且多为1型CNV, 约占扁平不规则PED的1/3[42]。此外OCTA也可用于评估CNV血流, 研究表明CSC患者存在明显的脉络膜血流异常, 并且脉络膜缺血往往先于CNV的发生[41], 这让我们对CSC的疾病病理又有了新的认识。
2.2.4 其他各种原因引起的CNV 鉴于OCTA的优势, 其应用可推广到各种原因引起的CNV, 用于疾病的诊断与鉴别诊断。譬如高度近视眼患者的黄斑出血, 其原因可以是Brush膜破裂引起的单纯性出血, 也可以是CNV破裂所致, OCTA可以鉴别出血的原因[43, 44]。再譬如多灶性脉络膜炎, 该病存在两大病理特征:一是炎症, 二是继发的CNV[45, 46], 传统的检查手段往往不能很好地区分彼此, OCTA则可帮助鉴别, 指导治疗, 判断预后[47, 48]。
视网膜血管的阻塞通常可以通过其特征性的眼底表现而作出正确的诊断, 传统的血管造影技术则可以显示血管充盈的速度, 但是决定视力预后的视网膜缺血程度是我们更关注的问题。OCTA对视网膜动静脉阻塞患者的检查可谓有劣势也有优势, 最大的劣势是无法显示视网膜动静脉充盈的延迟, 并且检查范围小, 难以覆盖周边视网膜, 但OCTA的优势也不少, 除了无需造影剂便可显现传统造影可以显示的缺血和异常血管如微动脉瘤、血管扩张以及交通支外, 由于OCTA不受血管渗漏的影响, 所以反而可以更好显示无灌注区的范围, 并且还可以区分视网膜缺血的层次[49]。
虽然OCTA检查已经显示出无比的优越性, 但是目前它依然在两个方面无法替代传统的造影, 一是无法计算眼底血管的动态充盈时间, 二是无法评价血-视网膜屏障的功能, 无法判断血管的通透性。此外当前OCTA技术的局限性还表现在以下几个方面:①移动性伪影问题。由于OCTA检测的是移动信号, 因此被检查者眼球的运动就会造成移动性伪影。此外, 虽然我们认定血管里流动的血细胞是眼内唯一移动的物质, 但是眼内渗出性的液体也有可能造成移动伪迹。②浅层血管在RPE的投影问题。由于高反射的RPE存在镜面效应, 因此其上方视网膜血管可以投射到RPE上形成伪影。此外其他一些视网膜内高反射的病灶, 也同样可以产生投射性伪影。这些伪影需要通过特定软件处理来去除。③血流速度对血流成像的影响。过慢或过快的血流速度都会导致血流信号丢失而影响血流成像, 导致一些有血流的血管结构却不显示血流信号, 如大的视网膜大动脉瘤和息肉样病灶等。未来可以用特殊软件处理以获取流速过慢或过快的血流信号。④量化统计的局限性。目前的软件可以量化一定范围内有血流的血管密度, 但是无法量化血管内血流的速度, 信号强度也与流速无关。未来有望研发更多的量化统计软件来满足临床科研各种定量分析的需求。⑤扫描范围的局限性。目前OCTA的检测范围主要集中在后极部黄斑区, 虽然有时可以通过拼图弥补扫描范围过小的问题, 但扩大扫描范围往往会损失图像分辨率或使得检查时间更长, 未来需要更大扫描范围、更高分辨率和更快速度的OCTA系统来弥补现有的不足。⑥软件的局限性。未来需要更精准的分层软件、运动矫正和消除投射伪影的后处理软件来获得更完美的血流血管影像, 满足临床医师的需要。最后就扫描技术而言, 目前大部分OCTA仍采用谱域OCT技术, 但是由于扫频OCT的光源波长比谱域OCT的长, 穿透力更强, 可更好地穿透混浊的介质, 而没有明显的信号衰落, 并且不使用Enhanced depth imaging(EDI)技术也能清楚看到脉络膜甚至巩膜, 所以未来有可能会有更多的OCTA设备采用扫频OCT技术。
综上, OCTA的临床应用远不止上文所述, 它已经逐步走进我们的日常诊疗工作中, 如同20年前的OCT一样, 从慢慢渗入到如今让临床医师无比依赖。在不久的将来, 随着设备和软件的不断更新, 技术的进一步完善, OCTA也一定会成为我们临床诊断必不可少的利器。
利益冲突申明 本研究无任何利益冲突
作者贡献声明 俞素勤:参与选题、设计、收集数据, 资料的分析和解释, 撰写论文, 根据编辑部的修改意见进行修改。李欣馨:收集数据, 资料的分析和解释, 根据编辑部的修改意见进行修改。许迅:对文章的知识性内容作批评性审阅; 行政、技术支持; 指导; 支持性贡献
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|