{kind=link}
{kind=link}
圆锥角膜患者双眼角膜生物力学性能的对称性
[黄子旭, 王勤美, 俞阿勇, 包芳军, 舒宝, 黄锦海 ]
]
]
|
|


目的:应用超高频Scheimpflug角膜生物力学分析仪(CorVis-ST)评估双眼圆锥角膜患者角膜生物力学性能的对称性。方法:病例系列研究。于2013年12月至2015年7月间根据Amsler-Krumeich圆锥角膜分期标准诊断纳入温州医科大学附属眼视光医院视光门诊就诊的双眼圆锥角膜患者40例(80眼)。每只受试眼均使用CorVis-ST测量3次,得到10项生物力学参数及眼内压(IOP)、中央角膜厚度(CCT)等12项参数。双眼间差异分析采用Student's t检验和Mann-Whitney U检验,双眼一致性分析采用Bland-Altman方法。结果:12个CorVis-ST参数的双眼95%一致性界限分别为:第1次压平时间(AP1 T) -0.56 ~ 0.61 ms(Z=0.441,P=0.229),第1次压平长度-0.75 ~ 0.77 mm(t=-0.178,P=0.907),第1次压平速度-0.063 ~ 0.053 m/s(Z=-1.528,P=0.171),第2次压平时间(AP2 T)-1.01 ~0.84 ms(t=-0.848,P=0.269),第2次压平长度-0.96 ~ 1.02 mm(t=-0.342,P=0.715),第2次压平速度-0.22 ~ 0.22 m/s(t=-0.087,P=0.812),最大形变时间(T)-1.38 ~ 1.11 ms (Z=-1.170,P=0.162),最大形变峰间距-1.70 ~ 3.93 mm(Z=-3.321,P=0.001),最大形变曲率-2.30 ~ 2.74 mm(t=1.014,P=0.287),最大形变幅度-0.34 ~ 0.28 mm(t=-1.057,P=0.221),眼内压-3.61 ~ 3.91 mmHg(t=-1.152,P=0.267),CCT -136 ~ 152 μm(t=-0.698,P=0.323),双眼间差异除最大形变峰间距外均无统计学意义。对应的一致性比值分别为8.8%、45.0%、37.0%、4.6%、65.8%、50.0%、8.5%、78.8%、46.5%、29.1%、32.6%、32.3%。在12个参数值中,AP1 T、AP2 T、T一致性比值较小,双眼间有着较高的一致性。结论:AP1 T、AP2 T、T拥有较高的双眼间对称性,在应用CorVis-ST对圆锥角膜患者行角膜生物力学性能研究时,应考虑到双眼间角膜生物力学对称性对结果的影响。
Objective: To evaluate inter-corneal symmetry of biomechanical parameters in keratoconus patients as measured by an ultra-high frequency corneal visualization Scheimpflug technology (CorVis-ST).Methods: In this case series study, 40 bilateral keratoconus patients diagnosed with the Amsler-Krumeich keratoconus classification were recruited from December 2013 to July 2015 at the Optometry Outpatient of the Eye Hospital, Wenzhou Medical University. The same operator, using the same CorVis-ST instrument, measured each eye three times. Twelve inter-corneal parameters measured by the instrument were recorded, including 10 biomechanical parameters, intraocular pressure, and central corneal thickness. Student's t-test and Mann-Whitney U-test were used to compare inter-corneal differences, while inter-corneal agreement was evaluated by the Bland-Altman plot.Results: The 95% limits of agreement and agreement ratios of the 12 parameters were as follows: applanation 1 time (AP1 T), -0.56 - 0.61 ms (8.8%, Z=0.441, P=0.229); applanation 1 length, -0.75 - 0.77 mm (45.0%,t=-0.178, P=0.907); applanation 1 velocity, -0.063 - 0.053 m/s (37.0%, Z=-1.528, P=0.171); applanation 2 time (AP2 T), -1.01 - 0.84 ms (4.6%, t=-0.848, P=0.269); applanation 2 length, -0.96 - 1.02 mm (65.8%, t=-0.342, P=0.715); applanation 2 velocity, -0.22 - 0.22 m/s(50.0%, t=-0.087, P=0.812); maximum deformation time (T), -1.38 - 1.11 ms (8.5%, Z=-1.170, P=0.162); maximum deformation peak distance, -1.70 - 3.93 mm (78.8%, Z=-3.321, P=0.001); maximum deformation curvature, -2.30 - 2.74 mm (46.5%, t=1.014, P=0.287); maximum deformation amplitude, -0.34 - 0.28 mm (29.1%, t=-1.057, P=0.221); intraocular pressure, -3.61 - 3.91 mmHg (32.6%, t=-1.152, P=0.267); and central corneal thickness, -135.70 - 152.10 μm (32.3%, t=-0.698, P=0.323). Of all measured parameters, only AP1 T, AP2 T, and T had low agreement ratios, indicating high inter-corneal symmetry.Conclusions: In our study population of binocular keratoconus patients, the parameters AP1 T, AP2 T, and T had high inter-corneal symmetry. Research protocols using the CorVis-ST to study keratoconus should take these results into consideration during data analysis.
圆锥角膜(Keratoconus, KC)是一种以角膜非炎症性、进行性变薄及锥形膨隆为临床特征的疾病, 双眼同时或相继发病, 可致视力中度至重度受损[1], 并导致生活质量下降[2]。以往临床诊断主要依靠裂隙灯显微镜下可见的角膜形态学变化, 如Vogt条纹、Fleischer环、角膜瘢痕或角膜隆起[3, 4]; 或已出现异常的角膜形态学参数如角膜厚度变化速率、前表面高度、后表面高度等做出诊断。近年来, 随着眼反应分析仪(Ocular response analyzer, ORA)及应用超高频Scheimpflug技术的可视化角膜生物力学眼压分析仪(Corneal visualization Scheimpflug technology, CorVis-ST)的出现, 临床在体测量角膜生物力学已成为可能。已有研究报道, 相比正常组, KC患者有较高的角膜弹性及较低的硬度和角膜滞后量(Corneal hysteresis, CH)[5, 6, 7, 8]。
ORA可记录角膜形变过程中红外反射光信号强度变化[9], 从而提供角膜滞后量、角膜阻力因子(Corneal resistance factor, CRF)等参数, 但无法直接展示角膜形变过程。CorVis-ST采用的Scheimpflug成像技术是另一种角膜形变数据采集方法, 具有形变过程可视, 数据采集速率快(4 330帧/秒)、频率高的特点。由于KC发病率较低, 为扩大研究的样本量, 部分研究同时纳入KC患者的双眼[10, 11, 12]。现已有多项研究显示KC双眼形态学特征存在不对称性[13], 故KC相关形态学研究中同时纳入双眼对统计结果无明显影响。但目前尚未见有关KC患者双眼生物力学性能对称性的报道。本研究拟对双眼发病KC患者双眼生物力学参数的对称性进行探讨, 为今后有关研究的样本纳入提供参考依据。
选择2013年12月至2015年7月在温州医科大学附属眼视光医院视光门诊就诊的双眼KC患者。本研究遵守赫尔辛基宣言, 并已通过温州医科大学附属眼视光医院临床科研伦理委员会审批, 所有研究对象均按照相关要求签署知情同意书。
纳入标准:根据Amsler-Krumeich圆锥角膜分期标准[14, 15]即Ⅰ 期为偏心性变陡、近视和(或)散光< 5.00 D, 平均中央K值< 48.00 D, 可见Vogt条纹, 角膜仍透明; Ⅱ 期为近视和(或)散光5.00~8.00 D, 平均中央K值48.00~53.00 D, 无角膜瘢痕, 最薄角膜厚度≥ 400 μ m; Ⅲ 期为近视和(或)散光> 8.00~12.00 D, 平均中央K值> 53.00 D, 无角膜瘢痕, 最薄角膜厚度200~< 400 μ m; Ⅳ 期为屈光度不可测量, 平均中央K值> 55.00 D, 中央角膜瘢痕, 最薄角膜厚度< 200 μ m。见表1。
| 表1 Amsler-Krumeich圆锥角膜分期标准 Table 1 Amsler-Krumeich keratoconus classification |
排除标准:①硬性角膜接触镜停戴4周以上; ②软性角膜接触镜停戴2周以上; ③结果测不出或测量的实验数据不全; ④其他眼部活动性炎症、器质性病变及眼部外伤史、手术史; ⑤患有全身遗传病、精神疾病者; ⑥单眼发病的KC患者。
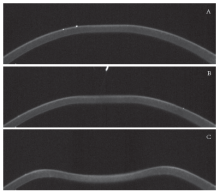
每位受检者均接受裸眼视力(Uncorrected visual acuity, UCVA)、最佳矫正视力(Best corrected visual acuity, BCVA)、主觉验光、裂隙灯显微镜、眼压测量等眼科检查, 其后行CorVis-ST(软件版本1.00r30, 德国Oculus公司)检查, 每只眼重复测量3次, 取平均值, 以上操作由同一位医师完成。CorVis-ST可记录气流脉冲作用下角膜第一次压平、最大形变及第二次压平直至恢复原始形态的全过程(见图1), 并通过分析形变图像得到10个角膜生物力学参数及眼内压(IOP)和中央角膜厚度(CCT)等数据。
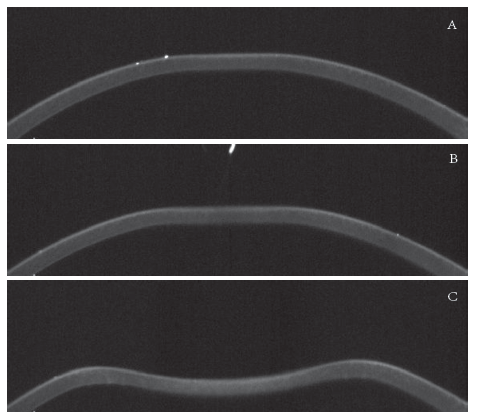 | 图1. CorVis-ST检查中角膜形变过程A:第一次压平阶段; B:最大形变期; C:第二次压平阶段Figure 1. Corneal deformation in CorVis-ST examination.A: Applanation 1 stage. B: Maximum deformation stage. C: Applanation 2 stage. |
各项检查均在受检者睡醒3 h后测量, 以减轻睡眠引起的角膜形态学变化对检查结果的影响[16]。进行CorVis-ST检查时, 受检者需端坐稳定, 下巴置于下颚托处, 额头靠于额托。检查过程中避免眨眼或闭眼, 受检眼注视仪器内视标, 操作者移动操作杆进行测量, 重复3次, 要求12个参数无缺失, 且“ 信赖性指数(Quality of scan, QS)” 参数显示为“ OK” , 否则重新进行测量, 如3次测量不达标则予以剔除。每次检查结束后休息2 min进行下一次检查。
CorVis-ST检查总共可提供12个参数, 包括IOP、CCT和10个角膜形变参数。根据所属的3个角膜形变阶段10个形变参数分别为:第一次压平阶段的压平1时间(Applanation 1 time, AP1 T)、压平1长度(Applanation 1 length, AP1 L)、压平1速度(Applanation 1 velocity, AP1 V), 第二次压平阶段的压平2时间(Applanation 2 time, AP2 T)、压平2长度(Applanation 2 length, AP2 L)、压平2速度(Applanation 2 velocity, AP2 V), 最大形变阶段的最大形变峰间距(Maximum deformation peak distance, PD)、最大形变幅度(Maximum deformation amplitude, A)、最大形变曲率(Maximum deformation curvature, C)及最大形变时间(Maximum deformation time, T)。
病例系列研究。使用PASW 22.0(美国SPSS公司)及MedCalc 11.4.2.0(比利时MedCalc Software公司)软件进行统计分析。所有计量资料均经单样本Kolmogorov-Smirnov正态性检验, 正态分布参数采用$\bar{x}$± s表示, 组间差异比较采用独立样本t检验; 非正态分布参数采用M (Q25, Q75)表示, 组间差异比较采用两独立样本的Mann-Whitney U检验。以P< 0.05为差异有统计学意义。双眼间生物力学参数对称性比较采用Bland-Altman法, 计算95%一致性区间(Limit of agreement, LoA)及一致性比值(95%LoA区间最大值的绝对值与总体均值比)评估其一致性。
研究共纳入40例双眼KC患者, 年龄15~67岁, 平均(31.5± 11.0)岁。患者左眼AP1 T、T、PD、IOP、CCT, 右眼AP1 V、T、PD、CCT呈非正态分布, 余参数呈正态分布。12个CorVis-ST参数中, PD为0.45(0.11, 2.62), 双眼间差异有统计学意义(t=-3.32, P=0.001), 余参数双眼间差异无统计学意义。双眼CorVis-ST参数值、分布范围、双眼间差异及一致性分析见表2。
| 表2 双眼圆锥角膜患者CorVis-ST参数的一致性分析 Table 2 Inter-corneal symmetry analyze of CorVis-ST parameters in bilateral keratoconus patients |
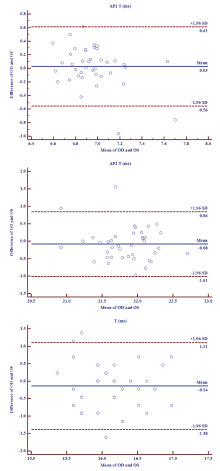
12个CorVis-ST参数的95%LoA分别为:AP1 T -0.56 ~ 0.61 ms, AP1 L -0.75 ~ 0.77 mm, AP1 V -0.063 ~ 0.053 m/s, AP2 T -1.01 ~ 0.84 ms, AP2 L -0.96 ~ 1.02 mm, AP2 V -0.22 ~ 0.22 m/s, T -1.38 ~ 1.11 ms, PD -1.70 ~ 3.93 mm, C -2.30 ~ 2.74 mm, A -0.34 ~ 0.28 mm, IOP -3.61 ~ 3.91 mmHg, CCT -136 ~ 152 μ m。对应的一致性比值分别为:8.8%、45.0%、37.0%、4.6%、65.8%、50.0%、8.5%、78.8%、46.5%、29.1%、32.6%、32.3%。在12个参数值中, AP1 T、AP2 T、T一致性比值较小, 双眼间有着较高的一致性(见图2)。其余9个参数, 由于双眼间差异的95%LoA较大, 临床工作中无法互相替代, 相关研究如同时纳入双眼数据将对最终统计结果无明显影响。
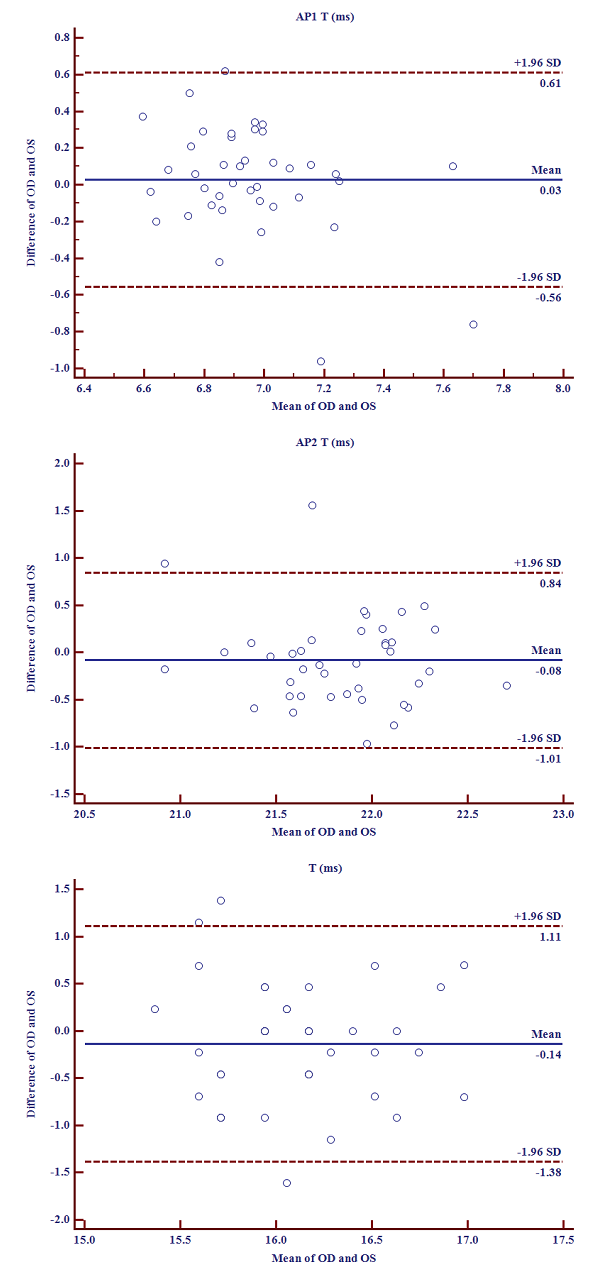 | 图2. 双眼圆锥角膜患者CorVis-ST参数的Bland-Altman图Figure 2. Bland-Altman plot of CorVis-ST parameters in bilateral keratoconus patients.OD, right eye; OS, left eye; AP1 T, applanation 1 time; AP2 T, applanation 2 time; T, maximum deformation time. |
根据双眼间KC分期差异将本组KC患者分为:A组:双眼KC分期相同, 共23例; B组:双眼KC分期差值为1, 共13例; C组:双眼KC分期差值为2或3, 共4例。3组受检者双眼间一致性分析结果见表3, C组双眼参数一致性比值较其他2组下降, 说明双眼间参数一致性随着KC分期差异增大呈下降趋势。
| 表3 不同分期双眼圆锥角膜患者双眼间CorVis-ST参数一致性分析 [80眼, $\bar{x}$± s / M(Q25, Q75)] Table 3 Inter-corneal symmetry of CorVis-ST parameters in bilateral keratoconus patients [80 eyes, $\bar{x}$± s / M(Q25, Q75)] |
KC是角膜屈光手术主要禁忌证之一, 常见双眼同时或相继发病, 人群患病率从0.002%到0.086﹪不等[17, 18]。单眼KC发病率仅占所有KC患者的0.5% ~ 4.0%[1, 19], 样本中仅纳入单眼KC患者往往难以达到样本量要求。部分研究为扩大研究样本量, 同时纳入KC患者的双眼[10, 11, 12]。由于当前KC患者双眼间生物力学性能的对称性缺乏临床研究结果, 故目前尚无法明确KC患者角膜生物力学的研究中纳入双眼是否会影响最终统计结果。
临床上多将单眼确诊KC而对侧眼未见明显症状的案例诊断为单眼KC, 但目前多数专家认为KC为双眼同时受累疾病[20, 21, 22, 23]。由于病源量少且随访难度大, 目前有关单眼KC的长期随访研究鲜见报道。Li等[24]于2004年报道了对85例单眼KC患者的随访研究(随访时长0.56~8.78年, 中位数时间3.4年), 发现30例单眼KC患者逐渐演变为双眼KC。而这30例患者中, 又有25例在初次确诊6年内发展为双眼KC, 表明KC为双眼发病, 但双眼间可能存在发病时间或临床特征的不对称性。
胶原纤维是角膜中主要蛋白成分, 约占角膜干重的70%, 含量丰富且排列规则, 是影响角膜光学性能及生物力学性能的重要结构。在KC患者, 由于基底层角膜上皮细胞降解导致蛋白水解酶含量增加, 进而导致Bowman层稳定性降低, 连续性中断[25]。相对正常人, KC患者角膜基质层胶原纤维层数量明显下降, 且锥顶区胶原纤维规则的正交排列发生紊乱[26]。此外, 胶原纤维间交联强度降低, 导致板层间稳定性下降, 使板层间相对滑动, 进行性变薄成为可能。这种病理改变的时间不对称可导致KC患者双眼先后发病, 同时可能造成双眼角膜生物力学性能的不对称。
Zheng等[27]应用ORA及离体全眼球膨胀平台对10只(20眼)健康兔的眼进行测量, 结果显示双眼间CH、CRF及角膜硬度差异均未见明显统计学意义, 双眼间生物力学性能存在较高的对称性。KC患者锥顶多位于旁中央区, 使用光电测量的ORA仅能测量角膜中央3 mm直径范围, 而CorVis-ST作为新一代角膜生物力学测量仪, 可测量8.5 mm角膜直径范围[28], 使其在KC患者角膜生物力学性能研究中有独特优势。此外CorVis-ST测量速度更快, 每秒钟可进行4 330帧扫描, 并可选取30 ms内的140张图像动态展示角膜形变过程, 可提供更为丰富的信息。本研究就双眼发病KC患者双眼间CorVis-ST参数对称性进行探讨, 首次证明了在双眼发病KC患者中, 双眼间AP1 T、AP2 T、T存在高度一致性, 这种情况在双眼KC分期差异较小的患者中尤为明显。因此, 在应用CorVis-ST对KC患者角膜生物力学性能进行研究时, 如同时纳入双眼发病KC患者的双眼, 在分析AP1 T、AP2 T、T时需注意双眼较高一致性对研究结果可能造成的影响。对于ORA参数是否存在类似结果本研究未证实, 有待进一步研究探讨。
综上所述, CorVis-ST的12个参数中, AP1 T、AP2 T、T拥有较高的双眼间对称性, 在应用CorVis-ST对KC患者角膜生物力学性能进行研究时, 应避免同时纳入上述双眼参数。
利益冲突申明 本文研究者声明本研究无利益冲突
作者贡献声明 黄子旭:参与课题设计, 收集数据, 资料分析及解释, 撰写论文, 根据编辑部的修改意见进行修改。王勤美、俞阿勇、包芳军:资料分析及解释, 参与修改论文中关键性结果、讨论。舒宝:参与收集数据。黄锦海:课题设计, 修改论文并参与对编辑部修改意见的修改
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|