{kind=link}
{kind=link}
{kind=link}
偏心和旋转对非球面Toric人工晶状体成像质量影响的实验研究
[张斌, 刘丹岩 , 柴茜楠, 魏玉华, 杜颖华, 段洁, 邢国献]
, 柴茜楠, 魏玉华, 杜颖华, 段洁, 邢国献]
, 柴茜楠, 魏玉华, 杜颖华, 段洁, 邢国献]
|
|


目的 通过对Toric人工晶状体(IOL)的球差进行自动优化,理论设计不同球差的Toric IOL,并且对其旋转、偏心的耐受性及成像规律进行研究。方法 实验研究。在模型眼中对Toric IOL球差进行优化,分别优化球面结构,IOL前、后表面曲率半径和厚度及Toric IOL的前表面非球面系数,目标设计获得-0.26、-0.1和0 μm球差的Toric IOL。在计算机光学模拟系统中,球面和非球面Toric IOL沿其X轴分别偏心0.25、0.50、0.75 mm,在3 mm和5 mm瞳孔直径下,评价其对调制传递函数(MTF)的影响;使其旋转3°、5°、10°,在4 mm瞳孔直径下评价其对MTF的影响。结果 在居中时随着瞳孔直径的增大,非球面Toric IOL成像质量下降低于球面Toric IOL;但在3 mm瞳孔偏心0.50 mm时,-0.26 μm的Toric IOL的成像质量下降并且低于0 μm和-0.1 μm的Toric IOL;5 mm瞳孔直径时偏心 0.75 mm,-0.26 μm球差Toric IOL的MTF与球面IOL接近,而0 μm和-0.1 μm球差的Toric IOL的MTF略优于球面Toric IOL。旋转3°和5°时,非球面Toric IOL MTF仍高于球面IOL;旋转10°时,非球面Toric IOL高空间频率的MTF已经接近或低于球面IOL。结论 -0.26 μm球差的Toric IOL居中时有良好的成像质量,但偏心耐受性较差。对Toric IOL球差的适量的优化,可以提高模型眼的成像质量,同时保持对偏心和旋转误差的耐受性,使其在综合条件下获得更好的光学质量。
Objective To optimize the spherical aberrations of toric intraocular lens (IOL): to design toric IOLs with different spherical aberrations, and to study the rotation, the tolerance to decentration, and imaging rules.Methods In this experimental study, the spherical aberrations of toric IOLs were optimized in the Hwey-Lan Liou model eye. The spherical structure, the curvature radius, and the thickness of the anterior and posterior surfaces of the toric IOLs, and the aspheric coefficients of the anterior surface of toric IOLs were optimized respectively. The targets was optimized to produce IOLs with -0.26 μm, -0.1 μm and 0 μm spherical aberrations. In the computer optical simulation system, the effect on the modulation transfer function (MTF) was evaluated when spherical and aspherical IOLs were decentrated in the horizontal direction with 0.25 mm, 0.50 mm and 0.75 mm at 3- and 5-mm pupil diameters. The effect on MTF was also evaluated when the two types of IOLs were rotated by 3°, 5° and 10° at 4-mm pupil diameter.Results: At the center, the aspherical toric IOL displayed a better image performance with the increased pupil diameter. When the decentration was 0.5 mm at 3-mm pupil diameters, the imaging quality of the -0.26 μm toric IOL decreased and was worse than that of 0 or -0.1 μm IOL. At 5-mm pupil diameter, when the decentration was 0.75 mm, the MTF of -0.26 μm toric IOL was close to that of the spherical toric IOL, while the MTF of toric IOL with 0 μm and -0.1 μm spherical aberration was slightly better than that of the spherical toric IOL. The MTF of aspherical toric IOLs was better than that of the spherical toric IOL with 3° to 5° rotation, but the curve was equal or even worse than that of the spherical toric IOL with 10° rotation in high spatial frequency.Conclusions:Toric IOLs with a spherical aberration of -0.26 μm have good imaging quality at the center but lower tolerance to decentration. The proper optimization of the spherical aberration of toric IOLs can improve the imaging quality of the model eye, while maintaining the tolerance for decentration and rotation errors. Optimized toric IOLs can attain better optical quality under comprehensive conditions.
伴有角膜散光的患者, 通过白内障摘除联合人工晶状体(IOL)植入可以有效矫正屈光不正[1], 但仍有部分患者感觉术后视觉质量欠佳。临床研究表明大部分患者角膜存在一定量的正球差[2], 由于自身晶状体在年轻时有一定量的负球差, 因此可以抵消部分角膜球差。而白内障手术后植入球面IOL会带来正的球差, 使IOL眼的总像差增大, 在一定程度上造成患者视觉质量降低。负球差的非球面IOL植入后就可以矫正角膜的正球差, 使视觉质量进一步提高[3]。但研究表明不同球差的非球面IOL对偏心的耐受性差异较大[4, 5]。Arcysof Toric IOL是基于球面设计的IOL, 植入眼内可带来正球差, 术后可引起全眼像差增大。对Toric IOL的观察表明, 植入术后IOL的轴位和角膜散光往往存在一定旋转偏差。本研究拟通过优化设计不同球差的Toric IOL, 并且在模型眼中进行光学模拟实验, 对其成像质量以及旋转、偏心对成像质量的影响进行探讨。
1.1.1 建立模型眼 参照文献[6, 7, 8]的方法, 应用Hwey-Lan Liou精密模型眼, 模拟使用Arcysof Toric IOL T4[6]。通过Zemax光学设计软件(ZEMAX Development Corporation, Bellevue, USA)建立模型眼, 设计使用+22.0 D的T4 Toric IOL的参数, 在光学模拟系统中, 使其后表面平坦轴置于X轴, 陡峭轴置于Y轴。模型在550 nm单色光条件下进行优化[9, 10, 11], 角膜前表面顶点至IOL前表面的距离设置为4.5 mm[12, 13, 14], 瞳孔直径设置为5 mm。
1.1.2 Toric IOL优化分为2个步骤进行[15]Toric IOL球面结构优化和球差优化[15, 16, 17, 18], 对+22.0 D的T4 Toric IOL的球面结构参数进行优化, 使其在球面结构时球差尽量减小。对Toric IOL前表面的Q值和高阶非球面系数进行优化。
根据公式[19]: 
z:IOL中心到表面极径的垂线距离
c:IOL表面的曲率
Q:非球面系数
a1:2阶非球面系数
a2:4阶非球面系数
优化目标:以Toric T4为基础, 使优化后的非球面IOL的球差分别为-0.26、-0.1、0 μ m。对IOL前表面Q值和2、4阶非球面系数进行自动优化。获得3种球差设计的非球面Toric IOL:T4a, 球差为-0.26 μ m; T4b, 球差为-0.1 μ m; T4c, 球差为0。
Toric T4、T4a、T4b、T4c IOL在模型眼中沿水平轴从中心逐渐偏心0.25 mm、0.50 mm、0.75 mm, 评价偏心在3 mm、5 mm瞳孔直径时对调制传递函数(Modulation transfer function, MTF)曲线的影响。4种IOL在模型眼中旋转3° 、5° 、10° , 评价旋转在4 mm瞳孔直径条件下对MTF曲线影响。光线追迹方法计算函数变量, 使用Originpro 7.5制图软件(OriginLab Corporation, USA)绘制MTF曲线。
T4n后表面均为

| 表1 优化后+22.0 D非球面Toric IOL光学参数 Table 1 Optical parameters of optimized +22.0 diopter aspheric toric IOL |
2.2.1 偏心对非球面Toric IOL成像质量的影响
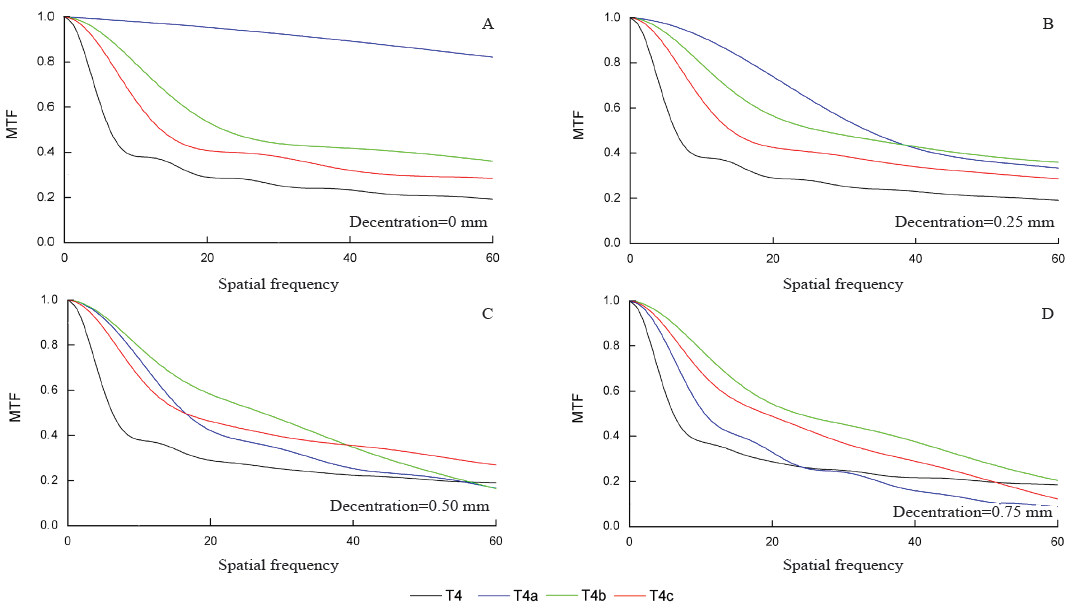
3 mm瞳孔直径条件下, IOL居中时, 非球面的T4a、T4b、T4c的MTF都明显优于球面T4 IOL, 3种非球面IOL的MTF在各空间频率都非常接近。当偏心0.25 mm时, 球面和非球面IOL的MTF较接近。当偏心达到0.50 mm时, T4a IOL的MTF降低较T4c IOL和T4b IOL明显, T4b IOL略优于T4c IOL, 但非球面Toric IOL的MTF仍然高于球面Toric IOL。当偏心0.75 mm, T4c IOL在中低空间频率的MTF优于其他IOL(见图1)。
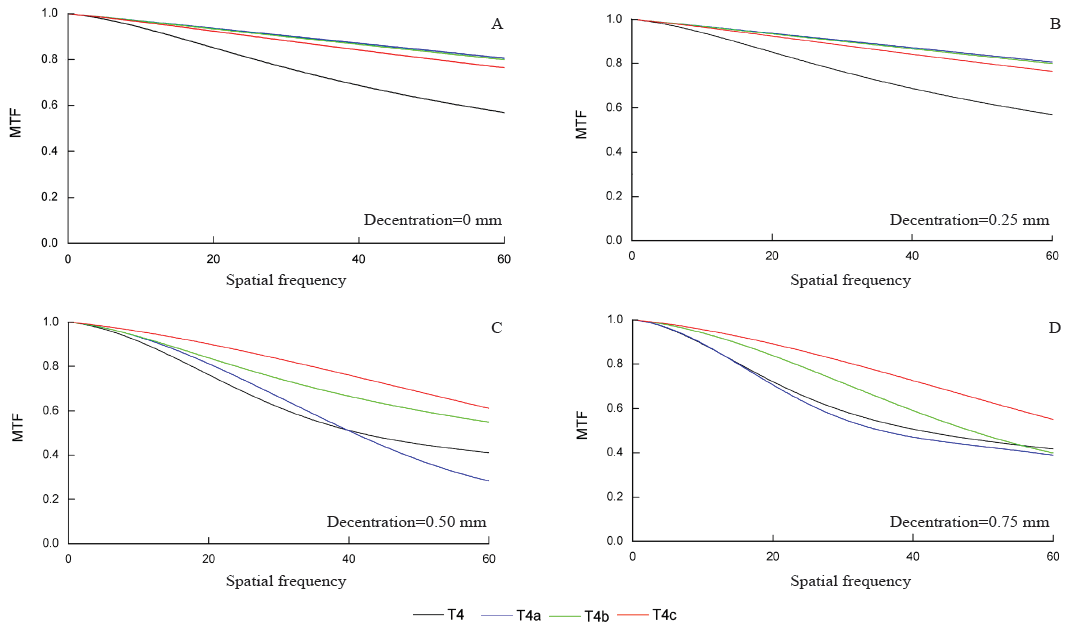 | 图1. 3 mm瞳孔直径条件下, 球面、非球面Toric IOL居中(A)及偏心0.25 mm(B)、0.50 mm(C)和0.75 mm(D)时MTF T4, 球面Toric IOL; T4a, -0.26 μ m球差Toric IOL; T4b, -0.1 μ m球差Toric IOL; T4c, 零球差Toric IOL; IOL, 人工晶状体; MTF, 调制传递函数Figure 1. With the 3 mm pupil diameter, the MTF of the spherical and aspheric toric IOLs were located in the center (A) and decentrated with 0.25 mm (B), 0.50 mm (C) and 0.75 mm (D), respectively. T4 IOL, spherical toric IOL; T4a toric IOL, with a spherical aberration of -0.26 μ m; T4b toric IOL, with a spherical aberration of -0.1 μ m; T4c toric IOL, with aberration-free. IOL, intraocular lens; MTF, modulation transfer function. |
5 mm瞳孔直径条件下, IOL居中时, 与3 mm瞳孔直径相比, T4a仍然保持良好的MTF, T4b MTF有明显降低, 但略优于T4c IOL, 而球面结构的T4 IOL MTF显著降低。当IOL偏心0.25 mm, T4a IOL MTF在中、低空间频率优于其他 IOL, 在高空间频率与T4b和T4c接近。当IOL偏心0.75 mm时, T4a的MTF已经与球面IOL接近, 此时T4b和T4c略优于T4a IOL(见图2)。
2.2.2 旋转对非球面复曲面IOL成像质量的影响 4 mm瞳孔直径条件下, IOL旋转3° 时, 非球面Toric IOL MTF没有明显降低, 仍高于球面IOL。旋转5° 时, 非球面Toric IOL MTF高空间频率降低更多, 但这个空间频率仍优于球面Toric IOL。旋转10° 时, 4种IOL 的MTF都进一步降低, 但3种非球面Toric IOL高空间频率的MTF已经接近或低于球面IOL(见图3)。
 | 图2. 5 mm瞳孔直径条件下, 球面、非球面Toric IOL居中(A)及偏心0.25 mm(B)、0.50 mm(C)和0.75 mm(D)时MTF T4, 球面Toric IOL; T4a, -0.26 μ m球差Toric IOL; T4b, -0.1 μ m球差Toric IOL; T4c, 零球差Toric IOL; IOL, 人工晶状体; MTF, 调制传递函数Figure 2. With the 5 mm pupil diameter, the MTF of the spherical and aspheric toric IOLs were located in the center (A) and decentrated with 0.25 mm (B), 0.50 mm (C) and 0.75 mm (D), respectively. T4 IOL, spherical toric IOL; T4a toric IOL, with a spherical aberration of -0.26 μ m; T4b toric IOL, with a spherical aberration of -0.1 μ m; T4c toric IOL, with aberration-free. IOL, intraocular lens; MTF, modulation transfer function. |
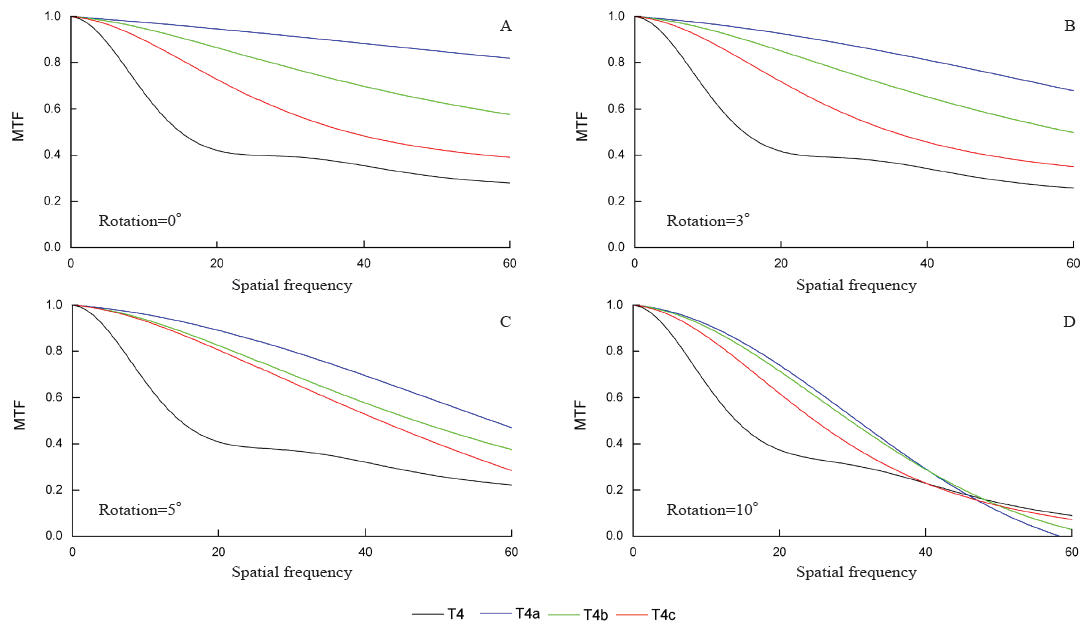 | 图3. 4 mm瞳孔直径条件下, 球面、非球面Toric IOL居中(A)及旋转3° (B)、5° (C)和10° (D)时MTF T4, 球面Toric IOL; T4a, -0.26 μ m球差Toric IOL; T4b, -0.1 μ m球差Toric IOL; T4c, 零球差Toric IOL; IOL, 人工晶状体; MTF, 调制传递函数Figure 3. With the 4 mm pupil diameter. The MTFs of spheric and aspheric toric IOLs were located in the center (A) and rotated by 3° (B), 5° (C) and 10° (D), respectively. T4 IOL, spherical toric IOL; T4a toric IOL, with a spherical aberration of -0.26 μ m; T4b toric IOL, with a spherical aberration of -0.1 μ m; T4c toric IOL, with aberration-free. IOL, intraocular lens; MTF, modulation transfer function. |
角膜和晶状体是人眼中最主要的屈光介质, 随着超声乳化人工晶状体植入手术的开展, 手术已经可以非常精确地矫正球镜度和柱镜度, 但IOL植入后可以带来全眼球像差的改变, 其中高阶像差主要是来自植入的IOL以及IOL偏心等因素引入的各种像差[20], 其中来自角膜的球差是主要的可以矫正的
高阶像差, 但很多研究表明, 由于角膜形态的个体差异以及不同的测量和计算方法, 文献报道不同样本的角膜球差数据个体差异很大。Holladay等[9]应用Obscan角膜地形图测量了71位白内障患者的角膜地形图, 使用格兰施密特正交拟合法对Zernike多形式的拟合, 计算角膜前表面的球差为(0.27± 0.02)μ m; Wang和Koch[21]测量228眼角膜球差为(0.28± 0.086)μ m; 有报道应用Pentacam前节分析系统测量角膜球差为(0.328± 0.132)μ m[22]。个体角膜的球差的不同一方面来自角膜的变异, 另一方面是由于测量和数据计算方法的差异以及是否综合计算角膜前、后表面的球差[23]。大量临床研究认为植入非球面IOL可使白内障患者术后全眼高阶像差降低, 视功能比植入球面IOL患者有大幅度提高[24]。
对IOL球差的优化可以提高术眼成像质量, 但也可能因倾斜、偏心等误差带来比较复杂的像差改变, 同时非球面Toric IOL可能增加散光轴位旋转带来的问题。人眼生理状态下, 植入眼内的IOL也有不同程度的偏心和倾斜。随着白内障手术技术的不断完善, IOL在眼内的居中性会越来越好, 但总会存在0.1~0.3 mm偏心, 2° ~6° 倾斜[25, 26]。本研究应用计算机光学模拟使用理论计算的方法, 试图探讨不同球差Toric IOL在多种误差条件下的成像质量, 探索合理的Toric IOL非球面优化。
居中时在各瞳孔直径条件下, T4a IOL成像质量明显好于其他球差的IOL, 并且随着瞳孔直径增大到5 mm, 零球差和-0.1 μ m球差IOL的MTF明显降低, T4a IOL这种优势更加明显。这是由于在本研究中-0.26 μ m球差的IOL完全抵消Hwey-Lan Liou模型眼中的角膜球差。Toto等[27]研究表明, Toric IOL植入不仅能矫正角膜散光, 还能降低患者全眼彗差。但与非球面IOL相似, 一旦出现偏心, -0.26 μ m球差的Toric T4a IOL的成像质量明显下降, 特别是在瞳孔直径5 mm时这种现象更为明显, 此时偏心0.5 mm T4a IOL的MTF 在所有空间频率已经低于-0.1 μ m球差的Toric IOL。Mckelvie等[28]研究了瞳孔大小、倾斜、偏心对3种非球面IOL的影响, 瞳孔大小是影响高阶像差的主要因素, 偏心是第二影响因素, 非球面IOL偏心0.5 mm以上会对高阶像差造成较大影响。非球面IOL在居中状态下可以抵消角膜球差, 改善视觉质量。非球面IOL偏心导致视觉质量降低的主要原因是离焦、散光、彗差的变化[29, 30, 31], 并且因球差大小不同而变化[32, 33, 34]。Altmann等[10]应用光线追迹实验对不同球差的IOL进行研究认为, 零球差和负球差的IOL在偏心0.5 mm和1 mm时出现非对称高阶像差, 造成成像质量降低, 但零球差的IOL受偏心影响较小。本研究表明在3 mm瞳孔时, 零球差IOL在不同偏心量时都有较稳定的成像质量, 5 mm瞳孔时由于-0.1 μ m球差的IOL球差较小, 但仍可抵消部分角膜球差提高成像质量, 也有较稳定的成像质量, 且略优于零球差IOL。Pé rez-Vives等[35]直接对不同屈光度的Acrysof IQ Toric IOL偏心时的波前像差的改变进行了研究, 但该测量没有设置相应的角膜模型, 随着偏心量的增大, 彗差增加, 但球差稳定不变, 当偏心0.6 mm时彗差增大可造成成像质量明显降低。彗差可能是单色像差造成视网膜成像质量下降的主要根源。
由于Toric IOL的偏心和旋转不引起球差的改变[35], 所以我们只在4 mm瞳孔直径条件下研究了非球面IOL的旋转对成像质量的影响。Toric IOL偏心、旋转对成像质量影响不同。Toric IOL偏心造成各空间频率MTF降低, 而旋转主要引起高空间频率MTF降低。Toric IOL旋转带来的主要是散光屈光度的增大和少量球镜度数的增加, 非球面Toric IOL的旋转与球面Toric IOL相同, 只造成散光的增加, 同样没有彗差、三叶草等非对称高阶像差的增加[6]。由于非球面Toric IOL抵消了部分球差, 所以在多数旋转的情况下MTF仍优于球面Toric IOL。
完全消除全眼球差的Toric IOL居中时有良好的成像质量, 在瞳孔大时表现更加优异, 但对偏心耐受性较差。对Toric IOL球差进行适量优化, 可以提高模型眼的成像质量, 同时保持对偏心和旋转误差的耐受性, 在综合情况下获得更好的光学质量。在我们前期的工作中对个体化模型眼在居中时球面和非球面IOL的成像质量进行了研究, 在本研究中分别对Toric IOL偏心和旋转的情况进行了分析, 但不足之处在于在临床的实际情况中, 偏心和旋转的误差是随机组合出现的, 非球面Toric IOL球差的优化及如何保持稳定的光学质量需要进一步探讨。
利益冲突申明 本研究无任何利益冲突
作者贡献声明 张斌:收集数据, 参与选题、设计、资料的分析和解释, 修改论文中关键性结果、结论, 撰写论文; 根据编辑部的修改意见进行核修。刘丹岩:参与选题、设计和修改论文的结果、结论; 根据编辑部的修改意见进行核修。柴茜楠、魏玉华、杜颖华、段洁、邢国献:参与资料的分析和解释; 根据编辑部的修改意见进行修改
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|