{kind=link}
IOLMaster700与IOLMaster500测量白内障术前眼轴长度的一致性及检出率比较
[崔蕊 , 杨文利, 李栋军, 王子杨, 陈伟, 赵琦, 李逸丰, 沈琳]
, 杨文利, 李栋军, 王子杨, 陈伟, 赵琦, 李逸丰, 沈琳]
, 杨文利, 李栋军, 王子杨, 陈伟, 赵琦, 李逸丰, 沈琳]
|
|


第一作者:崔蕊(ORCID:0000-0003-4116-7600),Email:cuirui_grace@163.com
目的比较新型扫频源生物测量仪IOLMaster700与传统部分相干光干涉生物测量仪IOLMaster500测量白内障患者眼轴长度(AL)的相关性、一致性及检出率。方法系列病例研究。选取2017年8-9月于北京同仁医院眼科就诊的年龄相关性白内障患者840例(840眼)纳入研究,分别应用IOLMaster700及IOLMaster500测量AL,2种仪器检出率差异采用 χ2检验进行比较,AL的数值差异采用配对 t检验进行比较,相关性采用Pearson相关分析,一致性采用Bland-Altman分析。结果IOLMaster700 AL检出率为93.4%,IOLMaster500 AL检出率为86.0%,二者差异具有统计学意义( χ2=63.00, P<0.001)。IOLMaster700及IOLMaster500测得的AL结果分别为(23.38±1.02)mm和(23.35±1.01)mm,差值为(0.03±0.04)mm,差异有统计学意义( t=-19.06, P<0.001),2种仪器测得的AL具有高度的相关性( r=1.00, P<0.001),Bland-Altamn分析95%一致性界限范围为0.13(-0.04~0.09)mm,上下限绝对值为0.09 mm,一致性较好。结论新型IOLMaster700与传统IOLMaster500测得的AL相比,具有高度相关性及良好的一致性,其检出率高于IOLMaster500,在白内障患者AL测量中具有一定优势。
Objective:To compare the agreement and success rate of axial length (AL) measurement between IOLMaster700, a novel swept source biometer, and IOLMaster500, a traditional partial coherence interferometry (PCI) optical biometer.Methods:In this case series study, 840 age related cataract patients (840 eyes) were enrolled in Beijing Tongren Hospital from August to September 2017. AL measurement was performed using IOLMaster700 and IOLMaster500 respectively. The differences of success rates between the two instruments were compared by χ2 test. The differences of AL were compared by paired t test. The correlations and agreement were analyzed by Pearson correlation analysis and Bland-Altman analysis.Results:The success rate of IOLMaster700 and IOLMaster500 were 93.4% and 86.0%, respectively. There was significant difference between the two methods ( χ2=63.00, P<0.001). The AL measured by IOLMaster700 and IOLMaster500 were 23.38±1.02 mm and 23.35±1.01 mm, respectively, with a difference of 0.03±0.04 mm ( t=-19.06, P<0.001). There was high correlation between two instruments ( r=1.00, P<0.001). The 95% agreement range of Bland-Altamn analysis was 0.13 (-0.04-0.09)mm. The absolute value of the upper and lower limit was 0.09 mm.Conclusions:Correlation and agreement between IOLMaster700 and IOLMaster500 are very high for AL measurements. Compared with IOLMaster500, IOLMaster700 has better AL measurement efficiency.
白内障术前准确的生物测量是选择合适人工晶状体度数, 减少术后屈光误差的重要保证。进行人工晶状体度数的计算需要的生物测量参数包括角膜曲率、前房深度及眼轴长度(Axial length, AL)等[1, 2, 3, 4], 研究报道术后屈光误差54%来自于AL, 所以更加准确的AL测量是白内障术后视力恢复的关键[5]。
IOLMaster检测AL精确性高、可重复性好、操作简便, 已成为临床上测量AL的金标准[6, 7, 8]。近日蔡司公司推出了更新版本的IOLMaster700, 区别于以往的生物测量仪, 该仪器利用扫频源相干断层成像(Swept-sourceoptical coherencetomography, SS-OCT)原理进行AL的测量, 使AL的测量更加直观准确[9]。本研究采用IOLMaster700与IOLMaster500测量AL, 比较2种仪器的检出率, 并分析二者的相关性及一致性, 以探讨IOLMaster700测量AL的临床应用价值。
选取2017年8-9月于北京同仁医院眼科临床确诊的年龄相关性白内障患者840例, 其中男349例, 女491例, 年龄为48~94(68± 10)岁, 选取每例患者的右眼数据进行分析。排除标准:①既往眼部手术史; ②合并眼部疾病, 包括视网膜脱离、眼内炎、玻璃体积血、高度近视、严重角膜或黄斑病变等。本研究符合赫尔辛基宣言, 所有患者均签署知情同意书。
所有患者依次应用IOLMaster500(德国Carl Zeiss公司, 软件版本3.02)及IOLMaster700(德国CarlZeiss公司, 软件版本1.5)进行测量, 测量方法:嘱患者将头置于额托, 操作者调整手柄将检测镜头对准患眼, 嘱患者注视镜头中红灯, 对焦清晰后进入AL测量界面, 采用自动模式测量获得AL结果。如AL测出, 且信噪比(Signal-to-noise ratio, SNR)大于1.6则认为AL检出。如首次未测出AL, 则再轻微调整镜头位置, 重复测量2次, 3次均未检出则认为AL未检出, 如重复测量时AL测出且SNR值大于1.6, 记为AL检出。测量结束后记录AL的数值。
系列病例研究。采用SPSS 22.0及MedCalc 16.2统计软件进行统计学分析。检出率为计数资料以率表示, 2种仪器AL检出率比较采用χ 2检验。AL为计量资料呈正态分布且方差齐, 以± s 表示, 2种仪器AL的数值差异采用配对t检验进行比较, 相关性采用Pearson相关分析, 一致性采用Bland-Altman分析。以P< 0.05为差异有统计学意义。
840只眼中, IOLMaster700能获得785只眼的AL数据, 检出率为93.4%, 检测的AL为(23.38± 1.02)mm; IOLMaster500能获得722只眼的AL数据, 检出率为86.0%, 检测的AL为(23.35± 1.01)mm。2种仪器AL的检出率差异具有统计学意义(χ 2=63.00, P< 0.001), 选择其中2种仪器均能获得AL的722只眼的AL比较, 结果显示差异具有统计学意义(t=-19.06, P< 0.001), 差值为(0.03± 0.04)mm。
2种仪器均能测得AL的722只眼的AL值进行相关性分析, 结果显示2组数据具有较高的相关性(r=1.00, P< 0.001)。2种方法测量AL95%一致性界限范围为0.13(-0.04~0.09)mm, 3.5%的点位于一致性界线以外, 上下限绝对值为0.09, 显示这2种设备检测AL数据的一致性良好, 见图1。
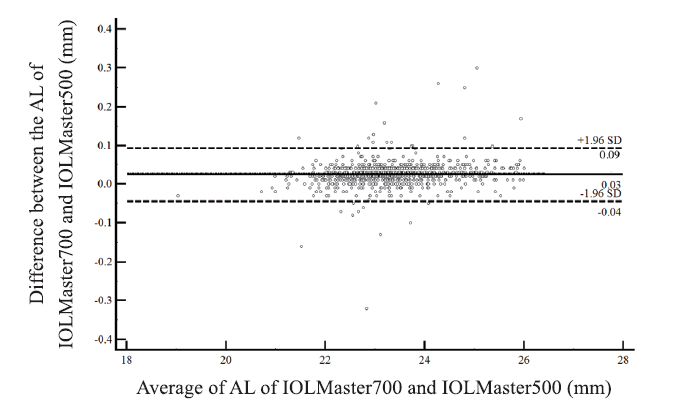 | 图1. IOLMaster700和IOLMaster500检测患者AL的Bland-Altman一致性分析 图中实线表示差值的均值, 虚线表示95%的一致性界限。Master700和IOLMaster500检测患者AL的95%一致性界限为-0.04~0.09 mm. AL, 眼轴长度Figure 1. Agreement of axial length between IOLMaster700 and IOLMaster500 by Bland-Altman analysis. The solid line in the figure shows the mean of the differences, the dotted line shows the 95% agreement limits. The 95% consistency limit of AL by IOLMaster700 and IOLMaster500 was -0.04-0.09 mm. AL, axial length. |
随着白内障摘除联合眼内人工晶状体植入手术的开展, 眼球的生物测量技术越来越受到临床上的重视[1, 2, 3, 4]。传统检测AL的方法为A型超声, 由于A型超声检测时探头直接接触角膜表面, 如果操作时对角膜造成压力, 会对检测结果的准确性造成影响。近年来多种光学生物测量仪相继问世, 由于不接触角膜, 解决了传统A型超声测量时可能压迫眼球的弊端, 且测量时患者注视固视灯, 直接测量角膜至黄斑中心凹的距离, 精确性高于A型超声, 为AL的测量提供了新的选择[10, 11, 12]。
IOLMaster作为最早应用于临床的光学生物测量仪, 在临床上应用广泛, 传统的IOLMaster500利用部分相干光干涉(Partial coherence interferometry, PCI)原理检测AL, 由于光线穿透力受屈光介质混浊程度的影响, 在严重混浊的白内障, 尤其是晶状体核性混浊和后囊混浊严重的白内障患者中, 其检出率较低[13, 14, 15]。当用光学生物测量仪不能检出AL的时候, 临床上只能应用A型超声, 所以提高光学生物测量仪检出率, 对于获得精准的AL至关重要。
本研究中IOLMaster700 AL的检出率为93.4%, 与IOLMaster500相比, 提高了AL的检出率。分析原因有2点:①光源不同:IOLMaster500利用780 nm的半导体激光作为光源, IOLMaster700光源为1 055 nm的可调节激光, 更长的波长增加了光线对组织的穿透能力, 从而提高AL检出能力; ②扫描方式不同:IOLMaster500仪器发出成束激光, 利用相干光干涉原理以A-scan方式进行视轴方向的单线扫描, 而IOLMaster700利用SS-OCT原理以B-scan方式进行眼球0° 、30° 、60° 、90° 、120° 、150° 6个方向的断层成像, 扫描范围更广, 也增加了AL检出能力[16]。Srivannaboon等[17]分别应用2种仪器测量了100例白内障患者的AL, 发现IOLMaster500 AL的检出率为95%, IOLMaster700检出率高达100%。同年, Akman等[18]对188只白内障眼进行AL测量, IOLMaster500 AL的检出率为91%, IOLMaster700检出率为100%, 并指出IOLMaster700在核性和后囊性白内障AL测量中更具优势。本研究测得2种仪器检出率分别为86.0%及93.4%, 低于国外研究, 这可能与国人传统观念和医疗条件限制, 白内障就诊较晚混浊程度较高有关。虽然2种仪器检出率都低于上述研究, 但IOLMaster700 AL的检出率高于IOLMaster500却是一致的, 均提示IOLMaster700在眼轴检出能力上具有优势。我们在裂隙灯显微镜下对IOLMaster500未检出、IOLMaster700检出以及2种仪器均未检出的患者晶状体混浊程度进行观察, 发现IOLMaster500未检出、IOLMaster700检出的患者白内障多处于膨胀期及成熟期, 而2种仪器均未检出的患者多为过熟期白内障, 提示IOLMaster700在膨胀期及成熟期患者的AL检出效率上与IOLMaster500相比更具优势。本研究中仅对部分特殊病例进行了裂隙灯显微镜观察, 并未客观地对所有患者进行国际分级并研究检出率及分级之间的相关性, 主观性较强, 这是本研究的局限性, 在今后的工作中我们将在本研究的基础上, 进行更深入、更客观的研究。
Bland-Altman结果显示, 2种方法测量AL的95%上下限绝对值为0.09 mm, Olsen[5, 19]指出0.01 mm的眼轴测量误差会导致0.03 D人工晶状体度数计算误差, 因此本研究中0.09 mm上下限绝对值仅导致0.27 D人工晶状体度数计算差异, 这种误差幅度在临床上可以接受, 且2种方法具有高度相关性, 95%的一致性界限也很窄(-0.04~0.09 mm), 故2种方法在临床上可以相互替代使用。Srivannaboon等[17]和Akman等[18]也发现2种仪器AL的测量值具有高度相关性及良好一致性, 与本研究结果一致, 但略有不同的是t检验比较2组AL差异无统计学意义。而本研究中显示二者AL, 有差异可能与本研究中部分患者固视状态欠佳有关。由于IOLMaster700可以直接观察到患者黄斑中心凹[20], 判断测量时患者固视状态, 所以我们认为当IOLMaster700与IOLMaster500测量结果不一致时, IOLMaster700的结果更为可信。
综上所述, IOLMaster700作为一种新型生物测量仪, 与IOLMaster500比较具有较好的相关性及一致性, 在临床上可以相互替代, 且具有检出率高、测量准确的优点, 比IOLMaster500更具有临床应用价值。
利益冲突申明 本研究无任何利益冲突
作者贡献声明 崔蕊:实施研究, 收集数据, 资料分析及解释, 撰写论文, 根据编辑部的修改意见进行修改。杨文利:酝酿和设计实验, 实施研究, 对文章的知识性内容作批评性审阅, 指导。李栋军、陈伟、王子杨、赵琦、李逸丰、沈琳:参与实施研究, 收集数据
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|