{kind=link}
{kind=link}
继发性淀粉样角膜变性的临床观察
[张子蓓 , 翟华蕾, 刘廷, 孔倩倩, 程钧]
, 翟华蕾, 刘廷, 孔倩倩, 程钧]
, 翟华蕾, 刘廷, 孔倩倩, 程钧]
|
|


第一作者:张子蓓(ORCID:0000-0002-7896-6783),Email:yfxx22b@163.com
目的 观察倒睫相关的继发性淀粉样角膜变性的临床特征。方法 回顾性系列病例研究。收集2014年1月至2015年12月期间在山东省眼科研究所青岛眼科医院接受治疗的倒睫相关的继发性淀粉样角膜变性患者的临床资料。对患者的年龄、性别、病史、临床表现、诊断方法、治疗和组织病理学检查结果进行总结分析。通过光学相干断层扫描(OCT)和超声生物显微镜(UBM)评估病变累及角膜的深度。结果 共纳入7例患者,其中男5例,女2例,年龄11~86岁。所有患者均有倒睫病史。角膜病变表现为单眼发病、角膜表面有新生物隆起,新生物具有表面欠平整、边界清晰和形状不规则等特征。OCT和UBM结果显示所有病例中病变深度均未累及后弹力层。有3例患者接受板层角膜移植术;1例患者行角膜病变切除联合羊膜覆盖术;3例患者行睑内翻及倒睫矫正术,因病灶对视力无明显影响,未行角膜病变切除术。组织病理学检查结果显示,角膜上皮下方有大量无定形的嗜酸性物质沉积,刚果红染色阳性,在偏振光下呈现“苹果绿”双折射现象。结论 与倒睫相关的继发性淀粉样角膜变性的临床特点主要表现为患眼同时存在倒睫及角膜新生物2种病变,且新生物的发病位置与倒睫刺激角膜的位置一致;角膜病变特点为倒睫刺激角膜的部位有新生物隆起,新生物表面欠平整,边界清晰、形状不规则。
Objective: To report clinical observations of secondary corneal amyloidosis (SCA) related to trichiasis diagnosed and treated at Qingdao Eye Hospital.Methods: In this retrospective series of case study, medical records of 7 patients with trichiasis-related SCA from January 2014 to December 2015 were reviewed. Patient age, gender, history of disease, clinical manifestation, diagnosis methods, treatments, and histopathological results were analyzed. The depth of amyloid deposition in the corneal stroma was examined with optical coherence tomography (OCT) or ultrasound biomicroscopy (UBM).Results: The patients were 5 males and 2 females, age 11-86 years. All patients had a history of trichiasis. The common characteristics of the corneal lesions were a unilateral and well-circumscribed mass, with an irregular and mulberry-like surface, protuberant from the corneal surface at the position irritated by trichiasis. OCT or UBM showed Descemet's membrane was uninvolved in all cases. Lamellar keratoplasties were performed for 3 patients, and 1 patient underwent lesion excision combined with amniotic membrane covering. For the other 3 patients, the entropion and trichiasis were corrected with surgeries, but the mass was not resected because visual acuity was not obviously affected. Amorphous eosinophilic materials, with positive Congo red stain and apple-green birefringence beneath the epithelium were revealed by histopathology.Conclusions: SCA related to trichiasis typically presents a unilateral, well-circumscribed, irregular, and mulberry-like mass protuberant from the corneal surface at the position irritated by trichiasis.
淀粉样角膜变性是一种罕见的眼部疾病, 表现为不溶性的淀粉样纤维蛋白沉积在角膜外基质内, 继而引起角膜结构和功能的异常。淀粉样角膜变性可分为原发性和继发性。其中, 原发性淀粉样角膜变性常见于某些角膜营养不良疾病, 比如格子状角膜营养不良和胶滴状角膜营养不良[1, 2, 3]; 而继发性淀粉样角膜变性与多种眼部疾病相关, 如倒睫[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]、圆锥角膜[16, 17]、眼部外伤[18, 19]、下睑赘皮[20]、边缘性角膜变性[21]、球形角膜[22]、角膜基质炎[23]和沙眼[24]。
第1例倒睫相关的淀粉样角膜变性于1969年被报道[4], 此后陆续有一些零星的报道[5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]。淀粉样角膜变性和倒睫常存在于同一只眼, 且角膜病变的发生位置与倒睫刺激角膜的位置一致。倒睫相关的继发性淀粉样角膜变性很罕见, 许多眼科医师对该疾病缺乏认识。因此, 本研究主要对山东省眼科研究所青岛眼科医院倒睫相关的淀粉样角膜变性患者的临床特征进行了回顾分析; 对手术切除的病变组织行病理学检查, 分析其组织病理学特征; 对目前已有的文献进行了回顾, 以提高广大眼科医师对该疾病的认识。
纳入标准:①患者合并倒睫或既往有倒睫病史; ②角膜表面新生物隆起, 其部位与倒睫刺激角膜的位置高度一致; ③角膜病变表现为新生物突起于角膜表面, 新生物边界清晰, 形态不规则。排除标准:①患有除倒睫以外的其他疾病者; ②其他病因明确的角膜新生物隆起者。
收集2014年1月至2015年12月期间于山东省眼科研究所青岛眼科医院诊断为倒睫相关的淀粉样角膜变性的患者。收集的患者信息包括年龄、性别、病史、病变表现、诊断、治疗和组织病理学结果等。
倒睫相关的淀粉样角膜变性的诊断基于以下检查结果:①根据纳入标准进行临床诊断; ②对于接受角膜病变切除术的患者, 术中取下的病变组织行组织病理学检查, 如在角膜上皮下有无定形的嗜酸性物质沉积, 刚果红染色阳性, 在偏振光下呈现“ 苹果绿” 双折射现象, 基本可明确病理诊断。
在裂隙灯显微镜下仔细观察淀粉样角膜变性的眼部病变表现。通过光学相干断层扫描(OCT)或超声生物显微镜(UBM)来检测病变累及角膜的深度及其下方未受累的角膜厚度。对于手术切除病变组织的患者, 术中切除的标本用10%的福尔马林液固定, 然后经过石蜡包埋、切片, 最后进行苏木素、伊红和刚果红染色。
对于倒睫尚未矫正的患者, 首先通过睑内翻矫正术或毛囊电解法尽早去除倒睫。视力受累明显的患者通过手术切除角膜病变组织, 病变累及角膜较深的患者联合板层角膜移植术, 病变相对表浅的患者联合羊膜移植术。病灶未对视轴造成明显影响的患者, 特别是要求暂不手术的患者, 病灶未予手术切除。
本研究共纳入7例患者, 其中男5例, 女2例。年龄11~86岁。角膜新生物存在的时间为2~30年。所有患者均无家族性眼病及眼部外伤史, 但均有倒睫病史。1例患者在来本院之前, 在其他医院已经进行了睑内翻和倒睫的矫正, 其他6例患者在本院就诊时均合并倒睫, 且倒睫刺激角膜的位置与角膜表面新生物的位置一致。在治疗方面, 我们首先去除了6例患者合并的倒睫。之后, 3例患者接受了病变切除联合板层角膜移植术, 1例患者接受了病变切除联合羊膜移植术。其他3例要求暂不手术, 未行手术治疗。
7例患者初诊视力均≤ 0.5, 眼压正常, 入院后行角膜OCT或UBM检查角膜新生物累及角膜的深度及其下方未受累区域最薄处的角膜厚度。根据角膜新生物下方未受累区域最薄处角膜厚度及新生物是否影响视力决定是否行手术治疗, 手术方式见表1。所有接受病变切除手术的患者, 术中取下的病变组织均行组织病理学检查, 结果均在角膜上皮下发现有大量无定形的嗜酸性物质沉积, 且刚果红染色阳性, 在偏振光下呈现“ 苹果绿” 双折射现象。见图1-2。
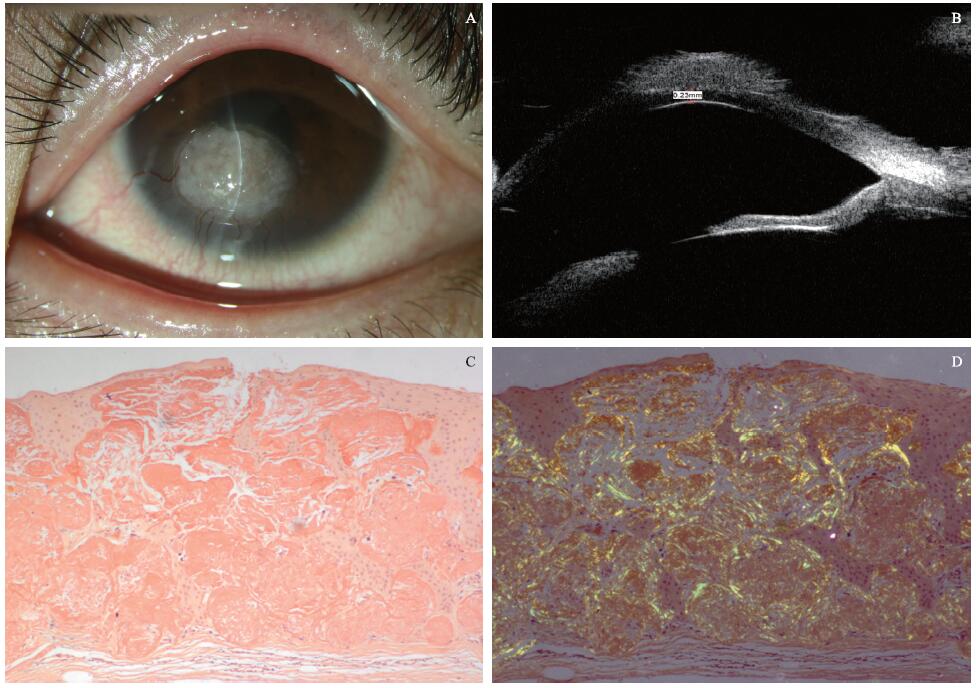 | 图1. 继发性淀粉样角膜变性患者1临床表现及检查结果 A:裂隙灯显微镜照相显示角膜表面新生物外观; B:同一眼的超声生物显微镜图像显示病变组织下方未累及的角膜厚度约230 μ m; C:组织病理学结果显示角膜上皮下发现大量无定形嗜酸性物质沉积, 刚果红染色阳性(× 400); D:在偏振光下呈“ 苹果绿” 双折射现象(× 400)Figure 1. Clinical manifestation and examinations of secondary corneal amyloidosis Patient 1. A: Slit-lamp photograph of the corneal amyloidosis mass. B: Ultrasound biomicroscopy image of the same eye showing that the thickness of the uninvolved cornea was about 230 μ m beneath the lesion. C: Histopathology revealed a large quantity of amorphous eosinophilic material deposited in the corneal stroma, with positive Congo red stain (× 400). D: Histopathology also revealed apple-green birefringence when viewed with polarized light (× 400). |
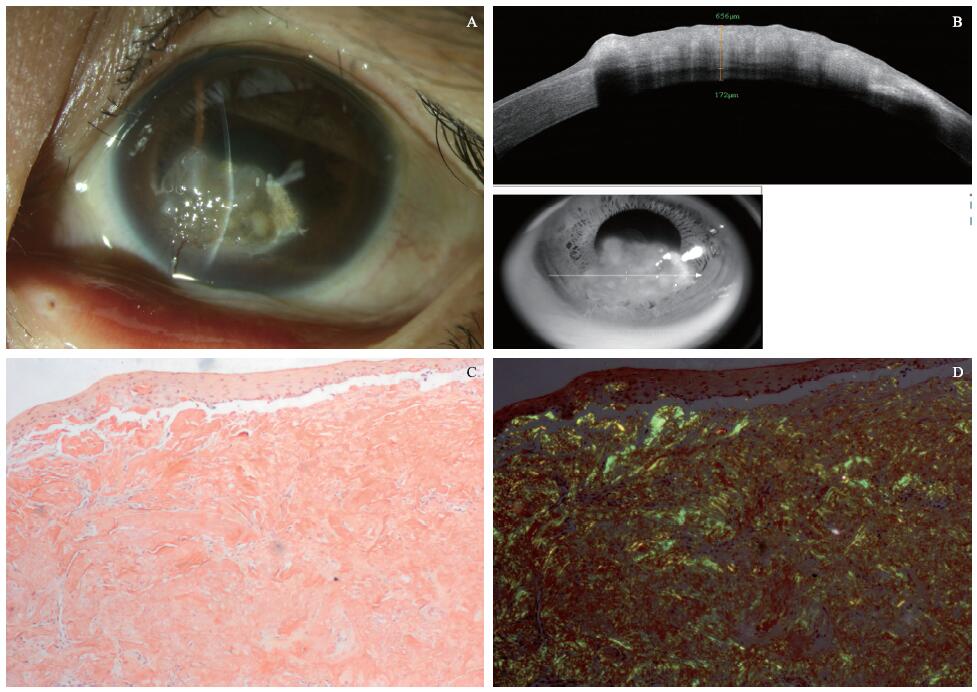 | 图2. 继发性淀粉样角膜变性患者3临床表现及检查结果 A:裂隙灯显微镜照相显示角膜隆起物外观; B:同一眼光学相干断层扫描图像显示病变组织下未受累的角膜厚度约172 μ m; C:组织病理学结果显示角膜上皮下发现大量嗜酸性物质沉积, 刚果红染色阳性(× 400); D:在偏振光下可见“ 苹果绿” 双折射现象(× 400)Figure 2. Clinical manifestation and examinations of secondary corneal amyloidosis Patient 3. A: Slit-lamp photograph of the corneal mass. B: Optical coherence tomography image of the same eye showed that the thickness of the uninvolved cornea was about 172 μ m beneath the lesion. C: Histopathology showed a large quantity of amorphous eosinophilic materials, with positive Congo red stain (× 400). D: Histopathology also revealed apple-green birefringence when viewed with polarized light, deposited beneath the corneal epithelium (× 400). |
| 表1 继发性淀粉样角膜变性患者初诊和治疗信息 Table 1 First visit and treatment of secondary corneal amyloidosis patients |
继发性淀粉样角膜变性通常为单侧发病, 且与眼部合并的一些其他疾病相关[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24]。尽管倒睫是文献报道中导致继发性淀粉样角膜变性最常见的因素[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15], 但倒睫相关的淀粉样角膜变性在临床上仍然非常罕见。通过查阅文献, 我们发现以往只有不到30例倒睫相关的淀粉样角膜变性的文献报道, 其中多数是亚洲人, 且不合并系统性疾病和家族史。
尽管倒睫和继发性淀粉样角膜变性之间的关系已有确定的报道[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15], 但是倒睫刺激引起角膜上皮下淀粉样蛋白沉积的过程仍不清楚。有人提出假说, 继发性淀粉样角膜变性的形成可能与患者的基因易感性有关。然而, 根据我们的临床观察和文献资料表明, 在同一个患者中, 即使患者双侧均有倒睫, 也只有单侧合并继发性淀粉样角膜变性, 这就提示倒睫导致的继发性淀粉样角膜变性可能与患者的基因易感性并不相关。在本研究中, 3例患者(患者2、3、7)有双眼倒睫, 但仅单侧发生了继发性淀粉样角膜变性的改变。
有研究证明, 眼表的慢性炎症刺激有可能导致淀粉样蛋白沉积于角膜基质内[19, 21, 25, 26, 27]。倒睫相关的继发性淀粉样角膜变性应该与角膜上皮的屏障受到破坏有关。上皮损伤由倒睫的机械刺激所引起, 角膜的上皮屏障被破坏后, 一些沉积在角膜表面的前体蛋白(例如乳铁蛋白[5, 6, 28, 29])会进入角膜上皮下, 并在此后促进继发性淀粉样角膜变性的发生。但是, 迄今为止继发性淀粉样角膜变性的发病过程仍不明确, 需要进一步深入研究。
有报道显示, 继发性淀粉样角膜变性的临床特征通常表现为单侧、表面不规则[12]、边界清楚的凝胶状肿瘤样物突起于角膜表面, 这与本研究中7例患者的临床表现完全一致。此外, 本研究的7例患者均存在新生血管自角膜缘长入的现象, 考虑新生血管的生长与倒睫的长期、反复刺激角膜相关。但是, 也有报道显示有少数倒睫相关的继发性淀粉样角膜变性的病例并不合并新生血管长入角膜[4, 10]。因此, 新生血管长入角膜并不是倒睫导致的继发性淀粉样角膜变性必要的临床表现特征。
组织切片行刚果红染色阳性和在偏振光下观察到“ 苹果绿” 双折射现象是淀粉样角膜变性特异性的病理表现和病理学诊断依据[30]。在本研究中, 4位患者切除的病变组织行病理学检查, 结果均可观察到位于角膜上皮下的无定形嗜酸性物质, 刚果红染色阳性, 在偏振光下呈现“ 苹果绿” 双折射现象, 这一特点是诊断淀粉样角膜变性的金标准[12]。但是对于一些病程处于早期、视力尚未明显受累的病例, 可能会因为患者拒绝手术而导致无法取得组织病理学标本。但是, 根据对该疾病特征的仔细观察及回顾分析, 我们发现同一眼合并倒睫与角膜新生物, 并且二者的发病位置高度一致对于诊断倒睫相关的继发性淀粉样角膜变性是必要的, 也是最重要的临床诊断依据。
由于倒睫和继发性淀粉样角膜变性之间的关系确切, 临床医师应在第一时间为患者去除倒睫, 以避免倒睫继续刺激角膜表面。倒睫去除后, 可再择期行角膜病变切除术, 并根据病变累及角膜的深度决定是否联合板层角膜移植术或羊膜移植术。对于没有症状、体积较小、不累及视轴区、比较表浅的淀粉样角膜变性病变不必急于切除, 但要嘱患者定期随访; 对于有明显刺激症状、病变范围大, 或者明显影响视力的患者, 应尽早行角膜病变切除术。
淀粉样角膜变性的手术方式根据淀粉样蛋白沉积在角膜基质中的深度来选择。根据我们的临床观察及文献报道, 倒睫相关的继发性淀粉样角膜变性患者的后弹力层很少受到淀粉样蛋白沉积的累及。因此, 对于病变较深, 累及后部角膜基质、但后弹力层并未受累的淀粉样角膜变性患者, 板层角膜移植术或深板层角膜移植术是理想的手术方式。对于病变较浅、病变范围较小的患者, 可以考虑准分子激光治疗性角膜切削术(Phototherapeutic keratectomy, PTK)或者单纯新生物切除术; 如果新生物切除面积较大, 建议联合羊膜覆盖术以促进术后角膜上皮的愈合。
OCT和UBM可以在活体内观察到角膜的细微结构。有很多研究报道可通过OCT或UBM在角膜疾病中观察角膜的形态结构[31, 32, 33, 34]。但是, 在之前的报道中, 仅有1个病例利用OCT检测角膜淀粉样蛋白在角膜中的沉积深度, 而UBM则没有相关报道。本研究中, OCT和UBM被用来确认淀粉样蛋白在角膜基质中的沉积深度以及病变下方未受累的正常角膜厚度, 这2项检查大大有助于临床医师根据病变深度为患者选择合适的手术方式。
倒睫相关的继发性淀粉样角膜变性是一种比较罕见的眼科疾病。本研究中第1例患者前来就诊时, 我们将其初步诊断为“ 角膜肿物” , 后来是根据组织病理学检查结果才得以确定诊断。另外6位患者在之后几个月相继来本院就诊, 通过临床观察和查阅文献, 很大程度上提高了我们对倒睫相关的继发性淀粉样角膜变性的认识。因此, 我们对这些病例资料进行了收集、整理, 可以为广大眼科医师提供参考。
综上所述, 倒睫相关的继发性角膜淀粉样变性的临床诊断主要根据倒睫刺激角膜的部位出现角膜新生物, 新生物表面呈现桑葚样外观, 边界清楚, 形态不规则。其组织病理学特征表现为角膜上皮下无定形的嗜酸性物质沉积, 刚果红染色阳性, 在偏振光下呈现“ 苹果绿” 双折射现象。所有患者的倒睫都应在第一时间去除, 之后可择期行准分子激光治疗性角膜切削术或角膜病变切除术, 根据病变累及角膜的深度和范围选择是否联合角膜移植或羊膜覆盖术。OCT和UBM可以检测角膜基质中淀粉样蛋白沉积的深度, 为临床医师根据病变深度选择合适的手术方式提供了有力的帮助。
利益冲突申明 本研究无任何利益冲突
作者贡献声明 张子蓓:收集数据, 撰写论文。翟华蕾:文章设计, 论文修改, 参与病例手术方案的制定及实施。刘廷:病理检查。谢立信:论文修改。孔倩倩:资料收集。程钧:参与病例手术方案的制定及实施
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|