{kind=link}
{kind=link}
{kind=link}
非球面Toric人工晶状体成像质量的蒙特卡洛分析
[张斌1  , 刘丹岩
, 刘丹岩1 , 柴茜楠1 , 杜颖华1 , 邢国献2 , 段洁3 ]
, 刘丹岩, 柴茜楠|
|


第一作者:张斌(ORCID:0000-0001-6625-8504),Email:1003695459@qq.com
目的 对Toric人工晶状体(IOL)的球差进行优化,并且对其旋转、偏心的耐受性及成像规律进行研究。方法 实验研究。使用计算机光学模拟在ZEMAX软件中对Toric IOL球差进行优化:①球面结构优化,分别优化IOL前、后表面的曲率半径和厚度。②Toric IOL球差的优化,设计优化目标分别为:-0.26、-0.1、0 μm球差的Toric IOL。在模型眼中,球面和非球面Toric IOL分别在3、4、5 mm瞳孔直径条件下随机偏心0~0.5 mm,旋转0°~5°,进行1 000次模拟,分别计算平均调制传递函数(MTF)、MTF的离散分布及蒙特卡洛分析。结果 MTF的离散分布:3 mm瞳孔时90%的情况下-0.1 μm和0 μm球差的Toric IOL的MTF分别≥0.77和≥0.78,优于-0.26 μm球差IOL的90%的测量值(≥0.55);5 mm瞳孔时90%的情况下-0.1 μm球差IOL≥0.35,0 μm的IOL≥0.29,优于-0.26 μm的IOL(≥0.16)。MTF的蒙特卡洛分析:3 mm瞳孔时,在大部分情况下-0.1 μm和0 μm球差Toric IOL都优于球面IOL,具有良好的可重复性;4 mm瞳孔时,3种非球面的Toric IOL几乎在所有情况下MTF都优于球面IOL;5 mm瞳孔时,在100%的情况-0.1 μm和0 μm球差非球面IOL的成像质量都优于球面IOL。-0.26 μm的非球面IOL对偏心和旋转的耐受性较差。结论 对Toric IOL球差的适量的优化,可以提高模型眼的成像质量并保持对误差条件下的耐受性,在综合情况下获得更好的光学质量。
Objective: To optimize spherical aberration with toric intraocular lens (IOL), to study the IOL tolerance for random rotation and decentration, and to delineate the image formation rules for toric IOLs.Methods: This was an experimental research. The spherical aberration for toric IOLs was optimized with ZEMAX optical design software. The following steps were taken: ①Adjust the curvature of the IOL spherical surface to minimize the target. ②Optimize the IOL front surface for -0.26 μm, -0.1 μm and 0 μm spherical aberrations. The modulation transfer functio (MTF) was analyzed with a discrete distribution and the Monte Carlo method at pupil diameters of 3 mm , 4 mm and 5 mm. A Monte Carlo simulation analysis with 1 000 trials with IOL decentrations of 0 mm to 0.5 mm and rotation from 0°-5° randomy.Results: There was a 90% discrete distribution of MTF with a 3 mm pupil: the spherical aberrations of -0.1 μm and 0 μm MTF were ≥0.77 and ≥0.78, respectively, which were superior to a -0.26 μm IOL ≥0.55. A 90% discrete distribution of MTF with a 5 mm pupil: a -0.1 μm IOL ≥0.35 and a 0 μm IOL ≥0.29 were superior to a -0.26 μm IOL ≥0.16. Monte Carlo simulation analysis of MTF: aspherical aberration of the toric IOL with a 3 mm pupil, either with 0.1 μm or 0 μm, showed superiority over a spherical IOL under most circumstances, with good repeatability. With a 4 mm pupil, all three types of aspherical toric IOLs had an advantage over a spherical IOL. With a 5 mm pupil, the spherical aberrations of a -0.1 μm and 0 μm toric IOL had an advantage over a spherical IOL under all circumstances. A -0.26 μm toric IOL had a lower tolerance for decentration and rotation.Conclusions: Appropriate adjustment and optimal spherical aberration of the toric IOL can improve imaging quality and tolerance under error conditions in a model eye, and better optical quality is obtained in general situations.
随着白内障手术技术的发展和人工晶状体(IOL)设计的不断完善, IOL植入可以有效矫正手术后球镜和柱镜的屈光度[1], 但研究表明大部分人的角膜有一定量的正球差[2], 自身晶状体在年轻时有一定量负球差, 可以抵消部分角膜球差, 而白内障手术后植入球面IOL会带来正的球差。虽然能准确矫正屈光度数, 但是球面IOL植入眼内引入的正球差使眼总像差增大, 这会在一定程度上造成患者术后视觉质量降低。负球差设计的非球面IOL植入后可以抵消患者角膜的正球差, 有效提高患者术后视觉质量[3]。临床测量表明, 即使在正常情况下IOL仍有0.3 mm偏心和3° 倾斜, 白内障术中良好的连续环形撕囊(Continuous circular capsu-lorhexis, CCC)技术可以使IOL获得良好的居中性, 但是由于悬韧带松弛或囊袋张力不对称等因素影响, IOL会平均偏心0.1~0.3 mm, 倾斜2.6° [4]。而IOL不同大小的球差对偏心的耐受性差异很大[5, 6]。Toric IOL和旋转对称的IOL术后一样可以存在不同程度偏心[7], 同时复曲面的特性还需要考虑到旋转对术后成像质量的影响。在临床条件下, 这2种因素是随机组合在一起的, 这就造成对其影响的评价较为困难。本研究拟通过优化设计不同球差的Toric IOL, 并且在模型眼中对偏心和旋转随机组合进行光学模拟研究, 探讨不同球差在随机误差条件下对成像质量的影响。
参照文献[8, 9]建立模型。应用Hwey-Lan Liou精密模型眼, 模拟使用Arcysof Toric IOL T4[8], 在ZEMAX光学设计软件(ZEMAX5.0, 美国 Zemax Development Corporation公司)建立散光模型眼, +22.0 D的T4 IOL后表面平坦轴置于X轴, 陡峭轴置于Y轴。
在ZEMAX光学设计软件模型眼, 瞳孔直径(Pupil diameter, PD)5 mm, 角膜前表面顶点至IOL前表面的距离设置为4.5 mm[10], 550 nm单色光条件下进行优化。
首先对Toric IOL球面进行优化:优化调整+22.0 D的T4 IOL的球面结构、厚度参数。以C04最小为目标进行优化, 使其IOL球差减小[11]。然后对Toric IOL前表面球差进行优化[11, 12], 根据公式[13]:
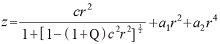
z:IOL中心到表面极径的垂线距离
r:极径
c:IOL表面的曲率
Q:非球面系数
a1:二阶非球面系数
a2:四阶非球面系数
优化目标:使Toric IOL T4的球差为-0.26 μ m、-0.1 μ m和0 μ m。使用自动优化, 对T4 IOL前表面Q值和2、4阶高阶非球面系数进行优化。获得3种球差设计的非球面复曲面IOL, 分别是T4a球差为-0.26 μ m(C04=0 μ m)、T4b球差为-0.1 μ m(C04=-0.16 μ m)和T4c为0 μ m(C04=-0.26 μ m)。
在模型眼中, Toric IOL T4、T4a、T4b、T4c 分别在3 mm、4 mm、5 mm瞳孔直径条件下各模拟IOL随机偏心0~0.5 mm, 旋转0° ~5° , 对512× 512条光线进行追踪, 光线追迹方法计算调制传递函数(Modulation transfer functio, MTF), 并进行1 000次模拟, 结果采用蒙特卡洛分析。
前表面:

其中$c=\frac{1}{-16.376}$
T4n后表面均为:
其中
$c_{x}=\frac{1}{-29.330}$
$c_{y}=\frac{1}{-29.392}$
2.2.1 非球面复曲面IOL MTF的离散分布 3 mm瞳孔时90%的情况下T4的MTF≥ 0.62, 高于T4a的≥ 0.55, 而T4b和T4c分别≥ 0.66和≥ 0.73, 优于T4a; 4 mm瞳孔时90%的情况下T4的MTF≥ 0.32, 与T4a的MTF≥ 0.32相同, 仍低于T4b和T4c的MTF≥ 0.49和≥ 0.43; 5 mm瞳孔时90%的情况下T4的MTF≥ 0.16, 与T4a的MTF≥ 0.16相同, T4b的MTF≥ 0.35, T4c的MTF≥ 0.29。见表1。
| 表1 球面和非球面Toric IOL在模型眼中MTF的离散分布 Table 1 The discrete distribution of MTF for aspherical and spherical toric IOLs in the schematic eye |
Toric IOL T4为球面IOL, Toric IOL T4a球差为-0.26 μ m, Toric IOL T4b球差为-0.1 μ m, Troic IOL T4c球差为 0 μ m
PD, pupil diameter; T4, Toric IOL T4, spherical IOL; T4a, Toric IOL T4a, spherical aberration is -0.26 μ m; T4b, Toric IOL T4b, spherical aberration is -0.1 μ m; T4c, Toric IOL T4c, spherical aberration is 0 μ m.
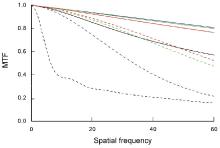
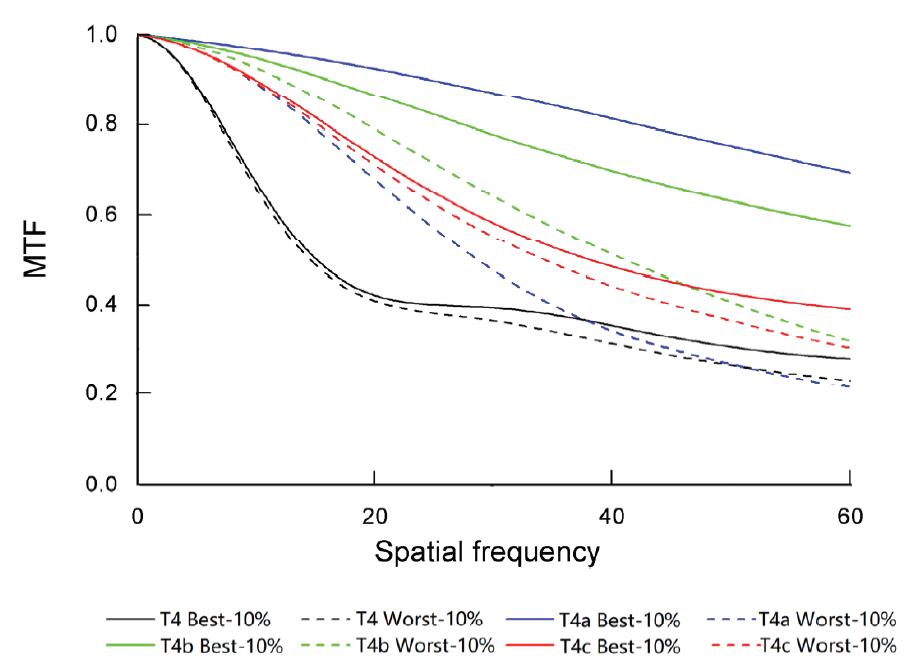
2.2.2 非球面复曲面IOL的蒙特卡洛分析 3 mm瞳孔时, T4a、T4b和T4c 3种非球面Toric IOL最佳10%MTF都优于球面T4。T4b和T4c最差10%MTF在大部分空间频率都接近或高于T4, 在大部分情况下这2种非球面Toric IOL都优于T4, 具有良好的可重复性。但T4a成像质量变化差异较大。见图1。
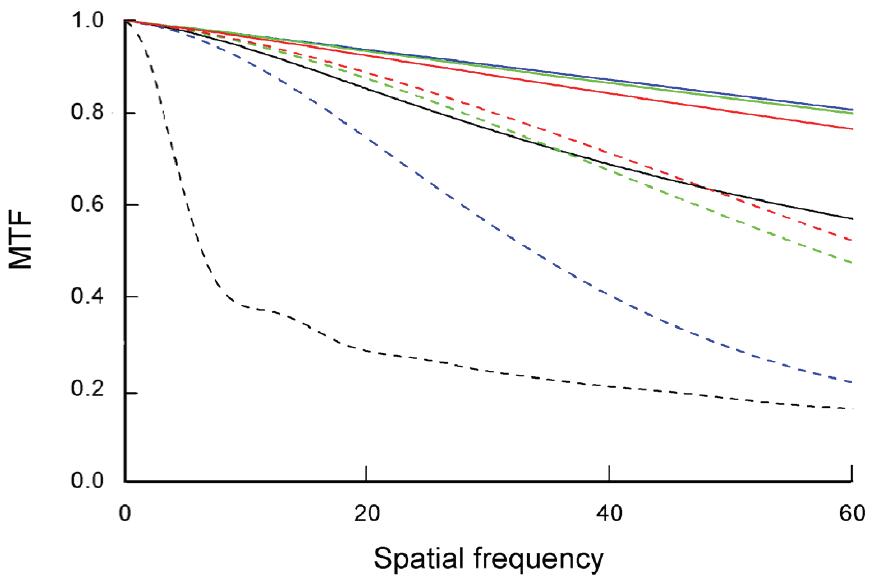 | 图1. 3 mm瞳孔时IOL模型眼蒙特卡洛分析最佳10%和最差10%的MTF曲线 IOL:人工晶状体; MTF:调制传递函数Figure 1. A Monte Carlo analysis for the best 10% and worst 10% MTF curves for a pseudophakic schematic eye with a 3 mm pupil. IOL, intraocular lens; MTF, modulation transfer function. |
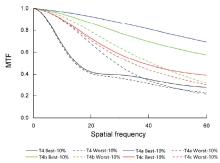
4 mm瞳孔时, T4 MTF曲线降低, 较3 mm瞳孔时成像质量下降, 最佳和最差10%MTF非常接近。T4a, T4b和T4c这3种非球面的Toric IOL几乎在所有情况下MTF都优于球面IOL。而T4a有10%的情况优于T4b和T4c。T4b和T4c耐受误差的情况较好, 最佳和最差10%的MTF曲线比较接近。T4b最差10%MTF在大多空间频率都优于T4c最佳10%MTF。见图2。
 | 图2. 4 mm瞳孔时IOL模型眼蒙特卡洛分析最佳10%和最差10%的MTF曲线 IOL:人工晶状体; MTF:调制传递函数Figure 2. A Monte Carlo analysis for the best 10% and worst 10% MTF curves for a pseudophakic schematic eye with a 4 mm pupil. IOL, intraocular lens; MTF, modulation transfer function. |
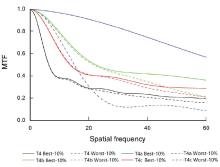
5 mm瞳孔时, T4 MTF曲线显著降低。T4b和T4c在所有空间频率时, 最差10%MTF都优于T4最佳10%MTF, 所以在100%的情况下T4b和T4c的成像质量都优于球面IOL, 而T4b略优于T4c。T4a有10%的情况优于T4b和T4c。T4a最差10%MTF在中高空间频率都低于T4最差10%MTF, T4a对偏心和旋转的耐受性较差。见图3。
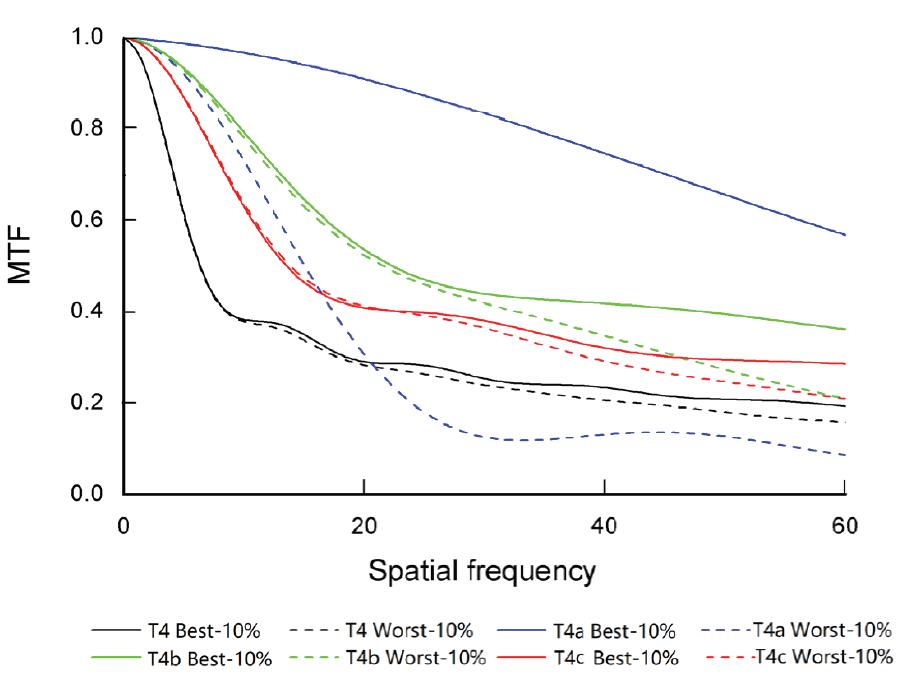 | 图3. 5 mm瞳孔时IOL模型眼蒙特卡洛分析最佳10%和最差10%的MTF曲线 IOL:人工晶状体; MTF:调制传递函数Figure 3. A Monte Carlo analysis for the best 10% and worst 10% MTF curves for a pseudophakic schematic eye with a 5 mm pupil. IOL, intraocular lens; MTF, modulation transfer function. |
研究表明, 由于角膜具有正球差, 但角膜形态的个体差异很大, 同时测量方法不同, 所获得的角膜球差数据有很大差异, 一般在0.27~0.33 μ m之间[14]。甚至角膜后表面的球差计算也会影响到角膜球差最后的结果[15]。
使用光学自适应系统的实验研究表明通过矫正球差, 可以使受试者的对比敏感度提高32%[16]。临床研究表明, 术中植入非球面IOL可以有效抵消角膜球差, 提高患者术后视觉质量[17]。术中植入非球面IOL可降低患者术后全眼高阶像差[18]。但非球面IOL偏心可以造成成像质量严重降低, 并且随IOL球差不同有很大差异。-0.27 μ m球差的IOL偏心> 0.5 mm时成像质量会低于球面IOL, 而0 μ m球差的IOL具有良好的误差耐受性[19]。白内障术中植入IOL的位置受到囊袋大小、悬韧带松弛、张力不对称等因素的影响, 这些可以造成IOL存在不同程度偏心[20]。Humbert等[7]对SN60T AcrySof(® ) Toric术后的测量旋转量为5.68° (0° ~14° ), 偏心为0.78 mm(0~1.78 mm), 而Toric IOL术后存在不同程度旋转偏差。所以本研究采用随机偏心0~0.5 mm、旋转0° ~5° 模拟临床情况进行分析。
全矫球差的非球面IOL在居中情况下有非常优良的成像质量。本研究对MTF的离散分布结果表明, 在3~5 mm瞳孔直径时有90%的情况下0 μ m球差和-0.1 μ m球差的IOL的MTF都高于-0.26 μ m的IOL, 这一分布提示全矫球差的Toric IOL在最优时有很高的MTF, 但其他情况下MTF可能比较低。彗差可能是造成非球面IOL视网膜成像质量下降的主要根源, 非球面IOL偏心导致MTF降低的主要原因是离焦、散光、彗差等改变[21]。对MTF的蒙特卡洛分析表明, 3 mm瞳孔时T4b和T4c IOL在大部分条件下都高于球面IOL, 具有良好的可重复性; 但T4最差10%MTF明显低于T4b和T4c最差10%MTF。4 mm瞳孔时T4a、T4b和T4c非球面的Toric IOL对角膜球差的矫正, 使其几乎在所有情况下MTF都优于球面IOL。5 mm瞳孔时T4b和T4c在所有空间频率的最差10%MTF都优于T4的最佳10%MTF。球差的矫正对提高IOL成像质量有明显效果, -0.26 μ m的T4a对角膜球差的充分矫正, 使其有10%的情况优于T4b和T4c, 但是T4a最差10%MTF在中高空间频率都低于球面IOL最差10%MTF, 提示-0.26 μ m球差的IOL对偏心和旋转误差的耐受性较差, 成像质量差异较大。球差对IOL非准直态误差的耐受性有较大差异[7]。Toric IOL偏心的特性和产生的影响与球面IOL相似[22]。有学者研究表明, Acrysof IQ Toric IOL偏心主要引起慧差的增加, -0.2 μ m Acrysof IQ Toric IOL在偏心大于0.6 mm时才引起MTF降低[7, 23]。
-0.26 μ m的非球面Toric IOL居中时有良好的成像质量, 在瞳孔增大时表现更加优异, 但对误差的耐受性较差。对Toric IOL球差的适量的优化, 可以提高模型眼的成像质量并保持对误差条件下的耐受性, 在综合情况下获得更好的光学质量。
利益冲突申明 本研究无任何利益冲突
作者贡献声明 张斌:收集数据, 参与选题、设计、资料的分析和解释, 修改论文中关键性结果、结论, 撰写论文; 根据编辑部的修改意见进行核修。刘丹岩:参与选题、设计和修改论文的结果、结论; 根据编辑部的修改意见进行核修。柴茜楠:参与资料的分析和解释; 根据编辑部的修改意见进行修改。杜颖华:参与资料的分析和解释, 参与修改论文中关键性结果、结论。邢国献、段洁:参与收集数据, 参与编辑部修改意见的修改
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|