
{kind=link}
{kind=link}
{kind=link}
OA-2000与IOLMaster 500、A型超声测量白内障眼部生物学参数的比较
[崇晓霞 , 王岩, 王盼, 云慧]
, 王岩, 王盼, 云慧]
, 王岩, 王盼, 云慧]
|
|


第一作者:崇晓霞(ORCID:0000-0003-1733-6670),Email:chongxiaoxia163@sohu.com
目的 比较最新的OA-2000光学生物测量仪与广泛应用的IOLMaster 500、A型超声测量白内障眼生物学参数的一致性。方法 系列病例研究。选取2018年5-6月内蒙古医科大学附属医院眼科确诊为年龄相关性白内障的患者152例(152眼),对所有患者依次采用OA-2000、IOLMaster 500、A型超声波(A超)这3种设备进行检查,获取眼轴长度(AL)、角膜曲率(Ks、Kf)、中央前房深度(ACD)、角膜横径(W-W)、中央角膜厚度(CCT)、晶状体厚度(LT)和人工晶状体(IOL)度数等参数。数据采用方差分析、Pearson相关分析及Bland-Altamn法进行分析。结果 ①OA-2000、IOLMaster 500、A超对AL和ACD的检出率分别为97.3%、78.2%、100%和99.3%、97.3%、100%;OA-2000、IOLMaster 500对Ks/Kf的检出率为99.3%、98.6%;对W-W的检出率为97.3%、94.7%。其中高度近视伴后巩膜葡萄肿且AL≥26 mm的17眼中,OA-2000、IOLMaster 500、A超对AL的检出率分别为88%(15/17)、65%(11/17)、100%(17/17)。②3种设备间测得的AL、ACD总体差异有统计学意义( F=12.63, P=0.02; F=10.57, P=0.01),其中OA-2000和IOLMaster 500测得的AL、ACD参数结果差异无统计学意义,A超与其他2种设备测得的AL、ACD差异均有统计学意义( P<0.001);OA-2000和IOLMaster 500测得的Ks/Kf、IOL、W-W参数差异均无统计学意义。③3种设备对AL测量的平均差值:OA-2000和IOLMaster 500为0.03 mm,OA-2000和A超为0.13 mm;3种设备对AL≥26 mm的AL测量的平均差值:OA-2000和IOLMaster 500为0.06 mm,OA-2000和A超为0.43 mm。④Pearson相关性分析显示OA-2000和IOLMaster 500在AL测量结果中具有较高的相关性( r=0.78, P=0.02)。⑤通过Bland-Altamn法对各设备的AL数据进行一致性分析,结果显示在95%的一致性范围内一致性良好。结论 OA-2000、IOLMaster 500、A超在白内障患眼中的眼部生物测量结果无差异,但OA-2000对AL的检出率明显高于IOLMaster 500,同时在高度近视伴后巩膜葡萄肿的AL测量中,OA-2000测量的精确性及可靠性更高。
Objective: To compare the consistency of OA-2000 with IOLMaster 500 and A-scan for biological measurements. The purpose of this study was to evaluate the measurements of OA-2000 in preoperative examinations of cataract patients.Methods: In this case series study, a total of 152 patients (152 eyes) diagnosed with age-related cataract were selected at the Affiliated Hospital of Nei Mongol Medical University from May to June 2018. All the patients were examined in turn by OA-2000, IOLMaster 500 and A-scan. Measurements by these three instruments were compared for axial length (AL), Ks/Kf, anterior chamber depth (ACD), white-to-white (W-W), lens thickness (LT) and intraocular lens (IOL) dioptor. The results were analyzed by one-way analysis of variance, Pearson correlation and Bland-Altman.Results: ①The detection rates of AL and ACD with OA-2000, IOLMaster 500, and A-scan were 97.3%, 78.2%, 100%, and 99.3%, 97.3%, 100%, respectively. The detection rates of Ks/Kf with OA-2000 and IOLMaster 500 were 99.3% and 98.6%. The detection rates of W-W with OA-2000 and IOLMaster 500 were 97.3% and 94.7%. Among them, 17 eyes had high myopia, posterior scleral grape swelling and an axial length≥26 mm. The detection rates of AL with OA-2000, IOLMaster 500 and A-scan were 88% (15/17), 65% (11/17), and 100% (17/17). ②There was a significant difference in AL and ACD between the three instruments ( F=12.63, P=0.02; F=10.57, P=0.01). The AL, ACD parameters measured by OA-2000 and IOLMaster 500 were not significantly different. There were significant differences in AL and ACD between A-scan and the other two instruments ( P<0.001). There were no significant differences in Ks/Kf, IOL or W-W parameters among the three instruments. ③The average difference in AL measurements between OA-2000 and IOLMaster 500 was 0.03 mm, between OA-2000 and A-scan was 0.13 mm. The average difference between the three instruments for AL measurements with an axial length≥26 mm: OA-2000 and IOLMaster 500 was 0.06 mm; OA-2000 and A-scan was 0.43 mm. ④A Pearson correlation analysis showed that there was a high correlation between the measured results of OA-2000 and IOLMaster 500 ( r=0.78, P=0.02). ⑤The consistency of AL results using Bland-Altamn analysis showed that there was good consistency in the range of 95% consistency. Conclusion: There was a high consistency in ocular biological measurements between the three instruments in cataract eyes. However, the detection rate of OA-2000 in AL was significantly higher than that of IOLMaster 500, and the accuracy of the OA-2000 measurement was obviously higher in the AL measurement in high myopia with posterior staphyloma.
随着眼科医疗水平的不断进步以及人们生活质量的提高, 人们对于视觉的要求不仅仅局限于裸眼视力的提高, 更注重视觉质量的提高, 这就要求眼部手术具有更高的质量, 而眼球生物参数的精确测量则是保证眼科手术高质量必不可少的因素。在白内障手术中, 眼轴长度(Axial length, AL)是精确计算人工晶状体(IOL)的基本参数。先前有研究报道AL参数在预测术后屈光不正方面起着至关重要的作用[1], 并对实际屈光误差有54.2%的影响[2]。中央前房深度(Anterior chamber depth, ACD)的精确测量在IOL的计算中也有着重要的作用[3]。超声生物测量由于其成本低、有效性高和操作方便, 一直以来是测量ACD、晶状体厚度(Len thickness, LT)和AL的常用方法。自IOLMaster 500问世以来, 光学生物测定由于非接触、操作性强、测量精准等优势, 逐渐在临床广泛应用并被视为眼科生物特征参数测量的金标准。新型非接触式光学生物测量仪OA-2000采用扫频OCT(Swept source OCT, SS-OCT)的原理, 具有成像速度快、分辨率高、穿透深度深等特点, 一次测量可以提供7个生物特征参数, 包括中央角膜厚度、ACD、AL、LT、角膜直径、瞳孔直径(包括2.5、3.0 mm)和角膜曲率。本研究旨在通过对白内障患者使用OA-2000、IOLMaster 500、A型超声这3种不同仪器进行眼部生物学测量, 并对各项参数的测量结果进行分析, 从而评价3种仪器间的差异性和一致性。
纳入标准:①确诊为年龄相关性白内障的患者; ②由同一位医师对患者进行眼前段及眼底检查; ③患者晶状体均为II-IV级混浊。
排除标准:无晶状体眼(或合并)、人工晶状体眼、玻璃体积血、视网膜脱离、玻璃体增生等疾病。
选取2018年5月1日至6月30日于内蒙古医科大学附属医院眼科住院行白内障超声乳化摘除及IOL植入手术的年龄相关性白内障患者152例(152眼), 年龄35~89(68.2± 2.4)岁。其中, 男62例(62眼), 女90例(90眼)。本研究符合赫尔辛基宣言, 所有患者均签署知情同意书。
依次采用OA-2000、IOLMaster 500、A超这3种不同设备进行检查。所有检查均由同一名经验丰富的眼科特检医师完成, 检查前与患者充分沟通, 检查过程中自然瞬目, 避免固视差、泪膜破裂等影响结果的因素。
1.2.1 A型超声 采用MD-2400S眼科A/B超声测量仪(天津迈达公司)进行测量。A超以视轴方向经过泪膜层、角膜中央前表面到达黄斑中心凹内界膜。通过浸润法获得AL、ACD、LT值, 由于A超不能测量角膜曲率, 所需的角膜曲率值由Topcon全自动电脑验光仪(日本Topcon公司)进行测量。
1.2.2 IOLMaster 500 采用光学生物测量仪IOLMaster 500(德国蔡司公司)进行测量, 该仪器基于部分相干干涉测量(Partial coherence interferometry, PCI)的原理, 扫描波长780 nm, 扫描深度为38 mm。通过扫描可以获得AL、角膜曲率K值(最陡峭径线Ks、最平坦径线Kf及平均值Km)、ACD、最大角膜横径白到白距离(White to white, W-W)、瞳孔直径(Pupil, P)。AL为自泪膜层至黄斑中心凹视网膜色素上皮层下的距离。
1.2.3 OA-2000 采用新型非接触式光学生物测量仪OA-2000(日本Tomey公司) 进行测量, 扫描波长为1 060 nm。根据检测眼混浊情况自动切换扫描范围, 水平3 mm, 垂直3 mm。测量时可获得中央角膜厚度(CCT)、AL、LT、ACD、Ks/Kf值(包括2.5 mm和3.0 mm)、P、W-W等数据。仪器自带13种IOL度数计算公式, 其中包括4种准分子激光原位角膜磨镜术(LASIK)术后计算公式。测量时, 以视轴顶点为圆心, 在直径1.5 mm范围内进行0° 、60° 、120° 、180° 扫描。设备根据患者情况自动选择扫描角度, 无需人工介入。
系列病例研究。采用SPSS 20.0软件进行统计学分析。数据符合正态分布, 以均数± 标准差表示。3种设备测得的参数比较采用方差分析, 两两比较采用LSD法。采用Pearson进行相关性分析。3种设备测量参数的一致性分析采用Bland-Altamn法。以P﹤0.05为差异有统计学意义。
OA-2000、IOLMaster 500、A超的AL检出率分别为97.3%、78.2%、100%; ACD为99.3%、97.3%、100%。OA-2000、IOLMaster 500对Ks/Kf的检出率分别为99.3%、98.6%; 对W-W的检出率为97.3%、94.7%。其中高度近视伴后巩膜葡萄肿且AL≥ 26 mm的17眼中, OA-2000、IOLMaster 500、A超的AL检出率分别为88%(15/17)、65%(11/17)、100%(17/17)。
3种设备测得的CCT、Ks/Kf、IOL、W-W结果差异均无统计学意义(均P> 0.05)。3种设备间测得的AL, ACD总体差异有统计学意义(F=12.63, P=0.02; F=10.57, P=0.01), 进一步两两比较, OA-2000和IOLMaster 500测得的AL、ACD参数结果差异无统计学意义(P> 0.05), A超与其他2种设备测得的AL、ACD差异均有统计学意义(P< 0.001), 见表1。
| 表1 OA-2000、IOLMaster 500、A超的眼部生物参数测量结果 Table 1 The biometric measurement parameters provided by OA-2000, IOLMaster 500 and A-scan (n=152) |
OA-2000和IOLMaster 500对AL测量的平均差值为0.03 mm, OA-2000和A超为0.13 mm。OA-2000和IOLMaster 500对AL≥ 26 mm的AL测量的平均差值为0.06 mm, OA-2000和A超为0.43 mm。
OA-2000、IOLMaster 500和A超测得的AL数据相关性分析显示IOL Master500测量值与OA-2000、A超测量值呈正相关(r=0.78, P=0.02; r=0.67, P=0.02); OA-2000测量值与A超测量值呈正相关(r= 0.60, P=0.01)。
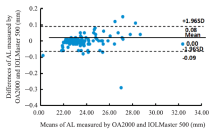
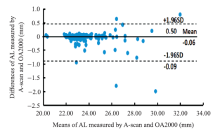
以2种设备所测AL的均值为横坐标, 差值为纵坐标建立Bland-Altman散点图。中间实线为2种设备所测AL差值的平均值, 该线上下两虚线表示其95%一致性界限(Limits of agreement, 95% LOA)。结果显示两两设备检测的AL数据在95%的一致性范围内一致性均良好。见图1-3。
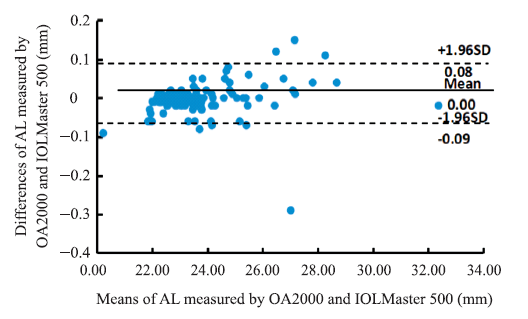 | 图1. OA-2000和IOLMaster 500测量AL的Bland-Altman分析图(152眼) 95%一致性界限内, 2种仪器测量值最大差值绝对值为0.29 mm。AL, 眼轴长度Figure 1. Bland-Altman plots show the agreement between OA-2000 and IOLMaster 500 for measuring axial length (152 eyes). In the range of 95% limits of agreement, the absolute value of the maximum difference between the two measurements is 0.29 mm. AL, axial length. |
 | 图2. OA-2000和A型超声测量AL的Bland-Altman分析图(152眼) 95%一致性界限内, 2种仪器测量值最大差值绝对值为0.8 mm。AL, 眼轴长度Figure 2. Bland-Altman plots show the agreement between OA-2000 and A-scan for measuring axial length (152 eyes). In the range of 95% limits of agreement, the absolute value of the maximum difference between the two measurements is 0.8 mm. AL, axial length. |
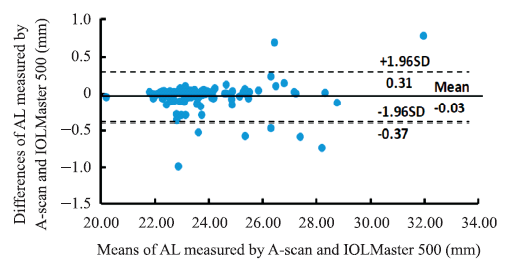 | 图3. IOL Master500和A型超声测量AL的Bland-Altman分析图(152眼) 95%一致性界限内, 2种仪器测量值最大差值绝对值为0.74 mm。AL, 眼轴长度Figure 3. Bland-Altman plots show the agreement between IOLMaster 500 and A-scan for measuring axial length (152 eyes). In the range of 95% limits of agreement, the absolute value of the maximum difference between the two measurements is 0.74 mm. AL, axial length. |
OA-2000应用SS-OCT的波长扫描激光光源, 以平衡探测型光电探测器来测量干涉光谱。OA-2000测量AL、ACD、CCT以及LT采用波长为1 060 nm的光学干涉波, 使用傅立叶域快速扫描OCT技术, 形成了“ B-扫描” 来完成各眼球参数的测量, 可以自动搜索晶状体的清晰界面, 避开晶状体的混浊部位。之前OA-l000应用了类似的技术, 但不能测量角膜曲率, 而新型生物测量仪OA-2000同时整合了Placido环角膜地形图技术, 可同时测量角膜直径2.5 mm及3.0 mm范围的角膜曲率, 并可记录Ks值、Kf值以及平均K值。最后通过红外线照射眼前节, 采用电荷耦合技术相机对眼前节参数进行采集, 经过软件分析和计算可获得瞳孔直径和角膜直径。当仪器开始启动, 就可以自动对焦, 自动完成对AL、ACD、CCT、LT等多项眼球参数的快速扫描。在测量过程中一旦探测到眼睑闭合等不符合要求的测量, 仪器将会自动重新进行测量。这样可以保证每次测得的参数符合要求。在既往的各类文献报道中, A型超声、Lenstar、IOLMaster 500均被认为可以为临床提供比较全面的生物测量参数, 测量的准确度也已经得到了很好的证实[4, 5, 6, 7, 8, 9, 10]。但目前国内的研究报道中, 似乎鲜有关于OA-2000在一些特殊的眼科手术如白内障手术术前检查中的测量与其他生物测量仪器进行比较, 鉴于以上OA-2000的多种优势, 为了解OA-2000与目前临床上已广泛使用的眼部生物测量仪器间测量结果的差异性, 我们进行了此次研究。
本研究的数据结果显示, 3种仪器获得的大部分参数, 特别是AL的一致性是比较好的。OA-2000与IOLMaster 500光学生物测量仪器所测量的AL结果误差非常小, 平均差值为0.03 mm。OA-2000和A超之间的平均差值为0.13 mm。根据SRK/T公式, AL中的0.08 mm的测量误差将导致0.20~0.34 D的误差, 0.10 mm的测量误差可能相当于0.25~0.30 D的误差。我们认为OA-2000与IOLMaster 500之间平均差值为0.03 mm, 在临床中被认为是可以接受的。
OA-2000与IOLMaster 500测定ACD、Ks/Kf、IOL、W-W的结果比较显示, 2种仪器间差异均无统计学意义。2种设备测量的AL、ACD、Ks、Kf、W-W、IOL的95% LoA分别为0.39 mm、0.31 mm、0.47、0.24、0.16和0.32 D, 表明这2种设备测量的生物参数结果的一致性是比较好的。
白内障同时伴有高度近视及后巩膜葡萄肿且AL≥ 26 mm的患眼由于易造成测量偏差, 因此测量结果的误差往往较大, 测量难度较高, 在本次研究中, AL检出率仍然以A超最高(100%), OA-2000为88.2%、IOLMaster 500为64.7%, 这也说明对于超长AL患眼的测量, A超仍然是最理想的手段。同时也可看出, 由于较好的穿透力, OA-2000的检出率的确高于IOLMaster 500, 可以更大程度地提高术前检查的精准度。
在本次研究中, 我们认为OA-2000相对于A型超声和IOLMaster 500是具有明显优势的, 同时在高度近视伴后巩膜葡萄肿的AL测量中, OA-2000测量的精确可靠性明显更高。与传统检查设备相比, OA-2000更好的穿透力和精准度可以更加优化常规及复杂白内障手术的效果。但本次研究也存在一定的局限性。首先, 本研究中使用的IOLMaster 500相对陈旧, 与IOLMaster 700相比, 可能会产生不同的结果。其次, 由于OA-2000临床使用的时间较短, 对其临床应用的确切作用以及在其他眼部疾病患者中的参数检出率及精准度等仍需进一步分析。
利益冲突申明 该研究对不同设备的测量进行了比较, 与仪器厂家无利益冲突
作者贡献声明 崇晓霞:收集数据; 资料分析及解释; 撰写论文。王岩、王盼:参与收集数据; 资料分析及解释; 修改论文。云慧:参与撰写论文; 修改论文中关键性结果、讨论
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|